
What Is Raynaud’s Phenomenon (RP)? Symptoms, Causes, Diagnosis & Treatment
Raynaud’s phenomenon (RP) is a condition in which very small blood vessels suddenly narrow too much in response to cold temperatures or emotional stress. This temporarily reduces blood flow, most often in the fingers and toes, and can cause color changes, numbness, tingling, pain, or coldness. Early evaluation can help distinguish harmless primary Raynaud’s from secondary Raynaud’s linked to autoimmune or vascular disease.
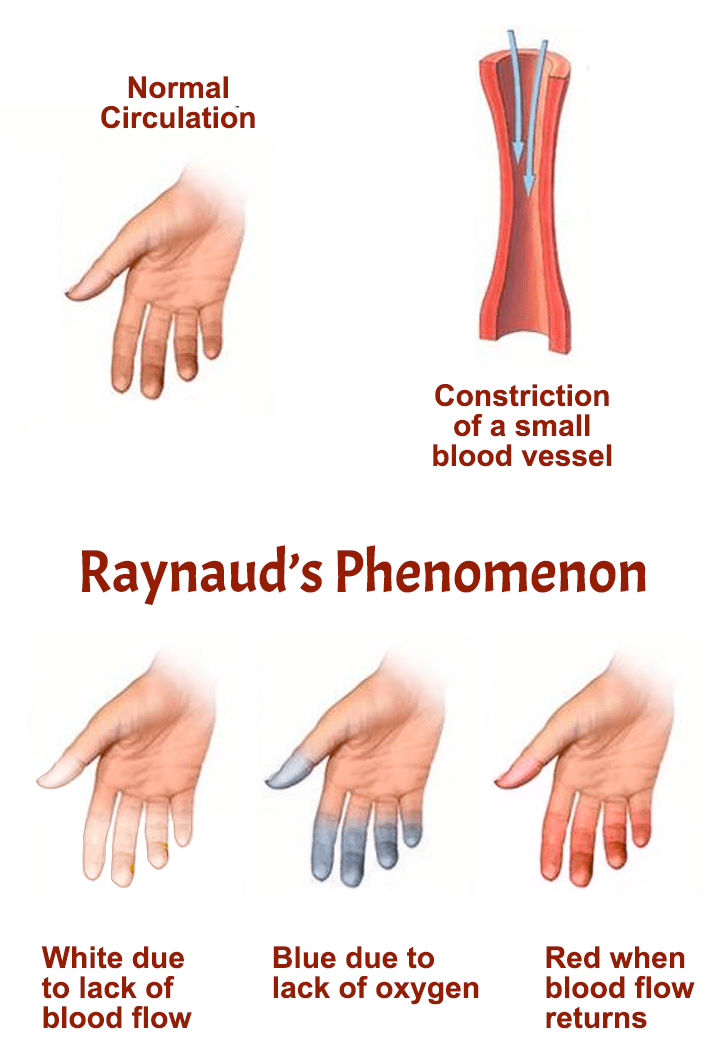
If you’re searching what is Raynaud’s phenomenon, the simplest answer is that RP is a circulation problem caused by episodes of exaggerated blood-vessel spasm. During an attack, the affected fingers or toes may turn white, then blue, and later red as blood flow returns. A rheumatologist can help confirm the diagnosis and create an individualized Raynaud’s treatment plan based on symptom severity, trigger pattern, and whether the condition appears primary or secondary.
Phenomenon
Raynaud’s often affects the fingers and toes, but it can also involve the ears, nose, or nipples in some people. Mild cases may mainly cause brief coldness and color change, while more severe secondary forms can lead to painful ulcers or tissue injury. Because Raynaud’s can be an early clue to connective tissue diseases such as scleroderma or lupus, getting the diagnosis right matters.
Table of Contents
- What Is Raynaud’s Phenomenon? Simple medical definition
- Raynaud’s at a glance
- Common Raynaud’s patterns
- Raynaud’s symptoms (what it feels like)
- Causes & risk factors
- How Raynaud’s is recognized
- Comorbidities & whole-body impact
- Prognosis (what to expect long-term)
- Understanding Raynaud’s: complete disease explanation
- Primary vs secondary Raynaud’s
- Diagnosis: exam, labs, testing
- Treatment: attack prevention + circulation protection
- Treatment targets (frequency, severity, tissue safety)
- Raynaud’s vs acrocyanosis (quick table)
- When to seek urgent care
- Downloadable Raynaud’s symptom checklist
- Related conditions (internal links)
- FAQs
- Conclusion + next steps
What Is Raynaud’s Phenomenon? Simple Medical Definition
Raynaud’s phenomenon (RP) is a vasospastic disorder in which small arteries and arterioles constrict too strongly in response to cold exposure or emotional stress. In short, clinically, what is Raynaud’s? It is a transient circulation disorder that causes episodes of reduced blood flow to the extremities, most often the fingers and toes, with color change, numbness, tingling, pain, and cold sensitivity.
Raynaud’s at a Glance
Cold-triggered attacks Symptoms often start after cold exposure or stress
Color changes Fingers or toes may turn white, blue, then red
Numbness or tingling Blood flow reduction can cause sensory symptoms
Primary or secondary Some cases occur alone, others are linked to autoimmune disease
Usually affects fingers Toes, ears, nose, and nipples can also be involved
Raynaud’s attacks are usually temporary, but severe secondary cases can damage tissue if blood flow is repeatedly impaired.
Common Raynaud’s Patterns
Raynaud’s is often divided into primary and secondary forms, but the clinical pattern can vary even within those categories. Some people have mild brief attacks only in cold weather, while others develop frequent painful episodes, ulcers, or symptoms linked to an autoimmune disease. Clinicians often think about Raynaud’s by trigger pattern, severity, symmetry, and whether there are signs of an underlying connective tissue disorder.
Primary Raynaud’s Usually milder, symmetric, and not linked to another disease
Secondary Raynaud’s Associated with autoimmune, vascular, medication, or occupational causes
Cold-dominant RP Mostly triggered by cold weather or cold objects
Stress-triggered RP Emotional stress strongly triggers attacks
Severe ischemic RP Painful attacks, ulcers, or tissue injury may occur
Raynaud’s symptoms (what it feels like)
Typical Raynaud’s symptoms include fingers or toes turning white or pale, then blue, then red as they warm up again. Attacks can cause numbness, tingling, throbbing, stinging, pain, or marked coldness in the affected areas. In more severe cases, especially secondary Raynaud’s, patients may develop persistent pain, fingertip sores, or delayed healing after repeated attacks.
Fingers • Toes • Ears • Nose • Nipples • Fingertips • Toetips
Cold, stress
Vasoconstrictors
Reduced blood flow
Color change
Cold, numbness
Pain, tingling
Primary vs secondary
Treatment plan
Wheel shows a simplified pathway: cold or stress trigger → vessel spasm → reduced blood flow → symptoms and long-term management.
Images for patient education
Finger color change

Cold-triggered vasospasm

Fingertip symptoms
Causes & risk factors
Raynaud’s happens because blood vessels overreact and constrict too much in response to triggers such as cold or emotional stress. Primary Raynaud’s occurs without another identified disease, while secondary Raynaud’s is linked to an underlying cause such as scleroderma, lupus, mixed connective tissue disease, thyroid disease, vascular disease, certain medications, smoking, or vibration exposure. The secondary form is usually more concerning because it may reflect structural blood-vessel damage or a broader autoimmune process.
- Cold exposure or sudden temperature changes
- Emotional stress
- Autoimmune disease such as scleroderma or lupus
- Smoking or nicotine exposure
- Certain medications that constrict blood vessels
- Repetitive vibration exposure or occupational trigger patterns
Evidence-based references (guidelines + high-quality sources)
General patient education: RheumInfo. Clinical overview: NIAMS. Professional review: NIH/NCBI StatPearls.
How Raynaud’s Is Recognized
Raynaud’s is recognized mainly from a classic story of episodic color change and cold sensitivity in the fingers or toes. Specialists often ask whether attacks are triggered by cold or stress, whether both hands are involved symmetrically, how long episodes last, and whether there are warning signs of an underlying autoimmune disease. The key clinical question is not only whether the person has Raynaud’s, but whether it is primary or secondary.
Typical white, blue, and red color changes
Triggered by cold or emotional stress
Numbness, tingling, pain, or cold digits during attacks
Recurrent episodes rather than one fixed discoloration
Clues to secondary disease such as ulcers, abnormal capillaries, or autoimmune symptoms
Comorbidities & whole-body impact
Raynaud’s can affect daily life far beyond temporary finger color changes. Frequent attacks may interfere with work, outdoor activity, sleep, exercise, fine motor tasks, and comfort in cold environments. In secondary Raynaud’s, clinicians also pay close attention to connective tissue disease, digital ulcer risk, blood-vessel damage, and broader autoimmune symptoms.
- Reduced hand function during attacks
- Pain or numbness that affects daily tasks
- Anxiety about cold exposure or recurrent episodes
- Fingertip sores or delayed healing in severe disease
- Underlying autoimmune disease such as scleroderma or lupus
- Rare tissue loss in severe ischemic cases
Prognosis (what to expect long-term)
The long-term outlook depends heavily on whether the condition is primary or secondary. Primary Raynaud’s is often manageable with trigger avoidance and may remain stable for years, while secondary Raynaud’s can be more severe and may worsen if the underlying disease progresses. The main goals are to reduce attacks, protect tissue, and identify any associated autoimmune or vascular disorder early.
Many mild cases improve with warmth and trigger control alone.
Severe secondary cases may need medication and close monitoring.
Good evaluation is important because Raynaud’s can sometimes be an early clue to another rheumatic disease.
Understanding Raynaud’s: Complete Disease Explanation
Raynaud’s happens when the small arteries supplying the skin suddenly clamp down more than they should. This reduces blood flow and produces the classic sequence of pallor, cyanosis, and then redness as blood flow returns. The attacks are temporary, but repeated episodes or underlying vessel damage can create more serious tissue problems in secondary disease.
What happens in the blood vessels?
In RP, a trigger such as cold exposure activates an exaggerated vasospastic response in the small blood vessels of the extremities. Reduced blood flow causes fingers or toes to become pale or white, then oxygen depletion can make them appear blue, and reperfusion causes the red recovery phase. This is why patients often describe a sequence of color change followed by throbbing or tingling as the digits warm up again.
Cold or stress trigger → sudden small-vessel spasm → reduced blood flow → white/blue color change → reperfusion with redness and tingling.
Primary vs secondary Raynaud’s
Primary Raynaud’s occurs on its own and is usually less severe, while secondary Raynaud’s is linked to another disease or external cause. Secondary Raynaud’s is more likely to cause pain, ulcers, tissue injury, abnormal nailfold capillaries, and positive autoimmune testing. This distinction matters because a person with secondary Raynaud’s may need treatment not only for the attacks but also for the underlying disease driving them.
Primary RP is often managed with warmth, trigger control, and monitoring.
Secondary RP may require autoimmune evaluation, medications, and ulcer prevention.
Correct classification helps guide both safety planning and long-term care.
Diagnosis: exam, labs, testing
Raynaud’s is diagnosed using the clinical pattern, history of attacks, physical exam, and targeted testing when secondary disease is suspected. Doctors may perform nailfold capillaroscopy to look for abnormal capillaries and order blood tests such as ANA, thyroid testing, or other autoimmune workup depending on the clinical picture. There is no single test that diagnoses every case, so the key is combining the attack history with examination and risk clues.
Tests often ordered during initial evaluation
Tests help separate primary from secondary disease and identify any linked condition.
- Detailed history of color change pattern, triggers, age of onset, and attack severity.
- Physical exam of the fingers, toes, skin, pulses, ulcers, and connective tissue disease signs.
- Nailfold capillaroscopy to assess capillary abnormalities.
- Blood tests such as ANA, thyroid testing, and selected autoimmune markers when indicated.
Treatment: attack prevention + circulation protection
Effective Raynaud’s treatment has two main goals: reduce the frequency and severity of attacks, and protect the skin and tissues from ischemic damage. For many patients, the first steps are non-medication strategies such as staying warm, avoiding sudden temperature exposure, stopping nicotine, and reducing trigger exposure. If symptoms are more severe or tissue injury is a risk, medications that improve blood flow may be needed.
1) Attack prevention (short-term control)
The first-line approach is usually practical trigger reduction. Gloves, hand warmers, warm socks, dressing in layers, avoiding cold objects, and stress management can make a major difference in mild cases. Patients should also avoid nicotine and other vasoconstricting exposures whenever possible.
2) Medical management (improving blood flow)
When lifestyle measures are not enough, calcium channel blockers such as nifedipine or amlodipine are commonly used as first-line medication treatment. Other vasodilating strategies may be considered in difficult or severe cases, especially in secondary Raynaud’s with ulcers or tissue-threat symptoms. The treatment plan depends on blood pressure, severity, ulcer risk, and whether the patient has an underlying autoimmune disease.
3) Lifestyle strategies that support treatment
- Keep the whole body warm, not just the hands, because core cooling can trigger attacks.
- Use gloves before touching cold objects such as freezer items or cold drinks.
- Stop smoking and avoid nicotine because it worsens blood-vessel constriction.
- Review medications with your clinician if any may worsen vasospasm.
- Seek reassessment if attacks become more painful, frequent, asymmetric, or associated with fingertip sores.
Treatment targets (frequency, severity, tissue safety)
In Raynaud’s, treatment targets focus on reducing attack frequency, shortening attack duration, lowering pain and numbness, and preventing fingertip injury. Clinicians track how often attacks occur, how long they last, whether there is skin breakdown, and whether an underlying disease is progressing. Good control means not just fewer color changes, but safer circulation and preserved tissue health.
| Target area | What your clinician tracks | What “on target” can look like |
|---|---|---|
| Attack frequency | How often attacks occur and what triggers them | Fewer episodes and better trigger control |
| Attack severity | Color change, numbness, pain, duration, rewarming difficulty | Shorter, less painful attacks |
| Tissue protection | Ulcers, sores, healing, ischemic pain, underlying autoimmune disease signs | No tissue damage and safer long-term circulation |
Case Study 1 (Example)
Patient experienced fingers turning white and blue in cold temperatures, followed by numbness and tingling. Evaluation suggested Raynaud’s phenomenon rather than poor- circulation or nerve compression.
Raynaud’s vs acrocyanosis (quick table)
Raynaud’s and acrocyanosis can both cause bluish color change in the extremities, but they are not the same condition. Raynaud’s causes episodic vasospasm with clear attacks and often white-blue-red color change, while acrocyanosis is usually more persistent, less painful, and not marked by distinct attacks. Distinguishing between them helps avoid confusion and ensures the right workup for secondary disease.
| Feature | Raynaud’s phenomenon | Acrocyanosis |
|---|---|---|
| Pattern | Episodic attacks | More persistent discoloration |
| Color sequence | Often white, blue, then red | Usually bluish discoloration without classic triphasic change |
| Trigger | Cold or stress | Often cold exposure, but less attack-like |
| Pain or numbness | Common during attacks | Usually milder |
| Tissue injury risk | Possible in severe secondary disease | Usually lower |
When to seek urgent care
- New fingertip sores, blackened skin, severe pain, or signs of tissue damage.
- Sudden asymmetric attacks, persistent ischemic pain, or symptoms that do not improve with warming.
- Raynaud’s symptoms plus chest pain, shortness of breath, or major autoimmune warning signs.
- Rapid worsening in someone with known scleroderma, lupus, or severe secondary Raynaud’s.
Call Now for Raynaud’s Phenomenon Care
⭐ Google Rating: 4.7/5 (184 reviews) • Insurance accepted: Most major plans (verify with office).
Patient testimonial: “My fingers kept turning white and blue in the cold and I didn’t know why. The team explained Raynaud’s clearly and helped me manage it better.”
Call Now: (352) 717-0603 Request AppointmentClinic Address
Rheumatology Care Associates PLLC (RCA)
2611 S US Hwy 27, Clermont, FL 34711
Email: info@rheumatologycareassociates.com
Office hours: Mon 8:30AM–5:00PM; Tue 8:30AM–5:00PM; Wed 8:00AM–3:30PM; Thu 8:30AM–5:00PM; Fri 9:00AM–1:30PM.
FAQ
Conclusion
Raynaud’s phenomenon is a common circulation disorder that can range from mild cold-triggered color changes to severe tissue-threatening ischemia in secondary disease. If your fingers or toes repeatedly turn white, blue, or red in response to cold or stress, a rheumatology evaluation can help determine whether the pattern is primary, secondary, or linked to an underlying autoimmune condition.
Disclaimer: This article is for educational purposes and does not replace professional medical advice. Always seek prompt care for fingertip sores, severe pain, or signs of tissue injury.
© 2026 Rheumatology Care Associates. All rights reserved.