Medically reviewed by Dr. Priya Prakash (Rheumatologist, board certified) | Last updated: March 20, 2026
What Is Giant Cell Arteritis (GCA)? Symptoms, Causes, Diagnosis & Treatment
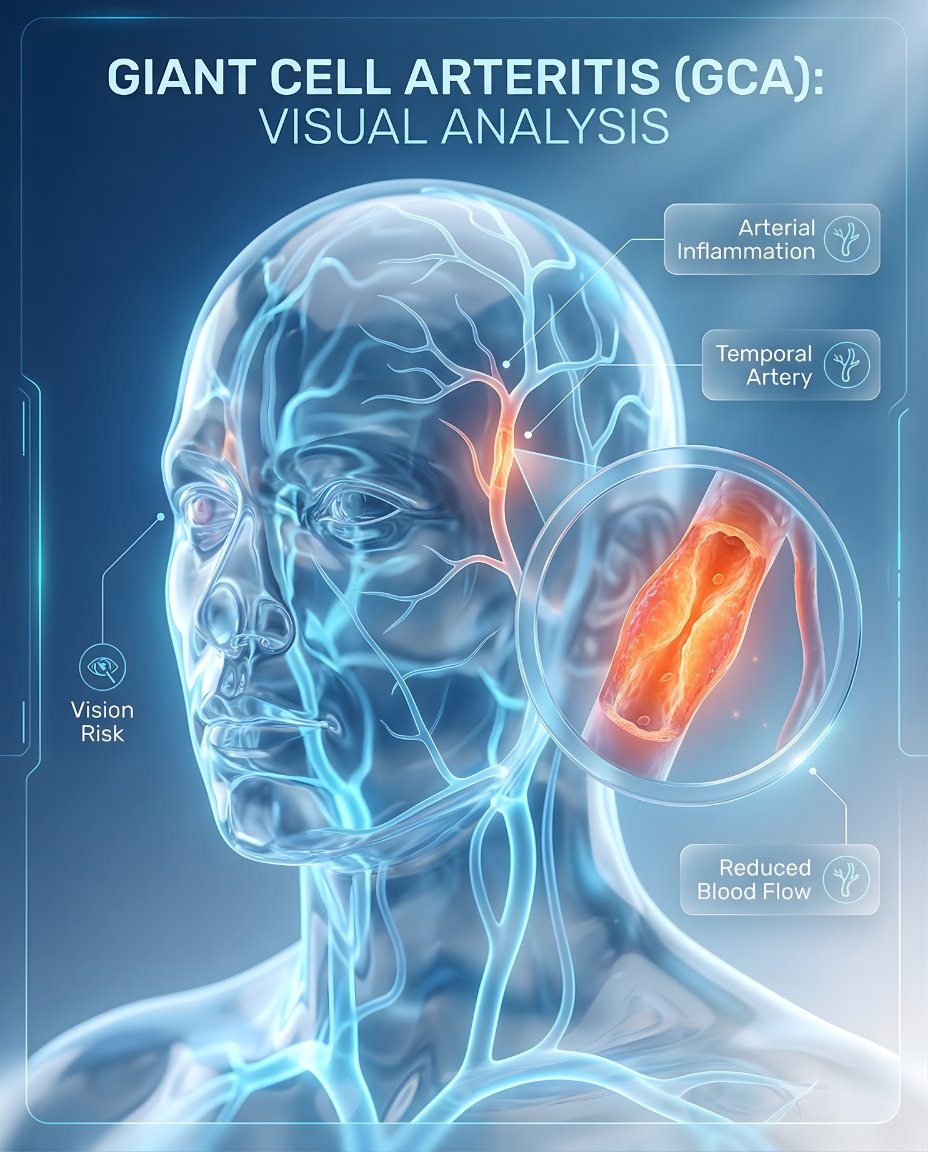
Giant cell arteritis (GCA), also called temporal arteritis, is an inflammatory disease of medium and large arteries. It often affects arteries around the head and temples, but it can also involve the aorta and other major vessels. Early diagnosis and immediate treatment are critical because GCA can cause sudden, permanent vision loss.
If you’re searching what is giant cell arteritis, the simplest answer is that GCA is a form of vasculitis in which inflamed artery walls narrow blood flow to important tissues. Many patients notice a new headache, scalp tenderness, jaw pain with chewing, or visual symptoms such as blurred or double vision. A rheumatologist must evaluate suspected GCA urgently and start a fast giant cell arteritis treatment plan to reduce the risk of blindness and other ischemic complications.
GCA is most often seen in adults older than 50 and is closely linked with polymyalgia rheumatica in some patients. Symptoms may also include fatigue, fever, weight loss, and tenderness over the temples. Because it is a vascular emergency when vision is threatened, getting the diagnosis right and acting quickly matters.
Table of Contents
- What Is Giant Cell Arteritis? Simple medical definition
- GCA at a glance
- Clinical patterns of giant cell arteritis
- Giant cell arteritis symptoms (what it feels like)
- Causes & risk factors
- How giant cell arteritis is recognized
- Comorbidities & whole-body risk
- Prognosis (what to expect long-term)
- Understanding giant cell arteritis: complete disease explanation
- GCA vs polymyalgia rheumatica
- Diagnosis: exam, labs, imaging
- Treatment: urgent control + disease management
- Treatment targets (vision and vessel protection)
- GCA vs migraine or tension headache (quick table)
- When to seek urgent care
- Downloadable GCA symptom checklist
- Related conditions (internal links)
- FAQs
- Conclusion + next steps
What Is Giant Cell Arteritis? Simple Medical Definition
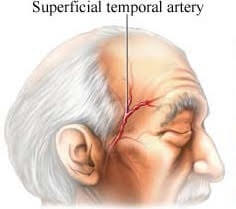
Giant cell arteritis (GCA) is a vasculitis that affects medium- and large-sized arteries, especially branches of the carotid arteries around the head. In short, clinically, what is GCA? It is an inflammatory blood-vessel disease that can reduce blood flow and cause headache, jaw claudication, scalp tenderness, visual symptoms, and in some cases major ischemic complications.
GCA at a Glance
New headache Often over the temples or scalp
Jaw claudication Pain or tiredness with chewing
Vision symptoms Blurred vision, double vision, or sudden loss
Scalp tenderness Pain when touching or combing hair
Age over 50 GCA typically affects older adults
Any visual symptom with suspected GCA should be treated as urgent because vision loss can become permanent.
Clinical Patterns of Giant Cell Arteritis
Giant cell arteritis can present with cranial symptoms, large-vessel symptoms, or both. Clinicians often think about whether the disease mainly affects the temporal and head arteries, whether the aorta or its major branches are involved, and whether polymyalgia rheumatica symptoms are also present.
Cranial GCA Headache, scalp tenderness, jaw pain, visual risk
Large-vessel GCA Aorta and major branches may be involved
PMR-associated pattern Shoulder and hip stiffness may coexist
Systemic inflammatory pattern Fatigue, fever, weight loss, malaise
Ischemic pattern Reduced blood flow can threaten vision or other tissues
Giant Cell Arteritis symptoms (what it feels like)
Typical giant cell arteritis symptoms include a new headache, temple pain, scalp tenderness, jaw pain while chewing, and visual symptoms. Some patients also have fatigue, fever, weight loss, neck pain, or symptoms of polymyalgia rheumatica such as shoulder and hip stiffness. Because GCA can suddenly reduce blood flow to the eye, new blurred vision, double vision, or vision loss is an emergency.
Temples • Scalp • Jaw • Eyes • Neck • Shoulders/hips (PMR overlap) • Large vessels
Age over 50
Immune activity
Artery walls
Reduced blood flow
Headache, jaw pain
Vision risk
Urgent diagnosis
Immediate treatment
Wheel shows a simplified pathway: artery inflammation → reduced blood flow → symptoms and urgent treatment.
Images for patient education
Temple headache
Artery inflammation
Vision warning
Causes & risk factors
The exact cause of GCA is not fully known, but it is considered an autoimmune inflammatory vasculitis affecting susceptible older adults. It predominantly affects people older than 50 years and is more common in some populations of older adults. The inflammation damages artery walls, narrows the vessel opening, and can reduce blood flow to tissues supplied by the affected arteries.
- New headache after age 50
- Scalp tenderness or temple pain
- Jaw pain or tiredness while chewing
- Blurred vision, double vision, or vision loss
- Polymyalgia rheumatica symptoms such as shoulder or hip stiffness
Evidence-based references (guidelines + high-quality sources)
General patient education: RheumInfo. Clinical overview: NIH/NCBI StatPearls. Diagnosis and treatment: Mayo Clinic.
How Giant Cell Arteritis Is Recognized
Giant cell arteritis is recognized using the clinical pattern, inflammatory markers, and confirmatory testing such as temporal artery ultrasound or biopsy. Specialists pay close attention to age over 50, new headache, scalp tenderness, jaw claudication, visual symptoms, elevated ESR or CRP, and imaging or biopsy evidence of inflamed arteries.
New headache after age 50
Jaw claudication or temple tenderness
Visual symptoms
Elevated ESR or CRP
Temporal artery ultrasound, biopsy, or vascular imaging support
Comorbidities & whole-body risk
GCA is not only a temple-headache disorder. It can involve large vessels such as the aorta and may be associated with aneurysm risk, stroke risk, or polymyalgia rheumatica symptoms in some patients. Good long-term care includes monitoring for vascular complications, relapse, and steroid-related treatment effects.
- Vision loss risk or other eye complications
- Polymyalgia rheumatica overlap
- Aortic or large-vessel involvement
- Stroke or ischemic complications in severe cases
- Fatigue, weight loss, and systemic inflammation
- Steroid-related side effects during treatment
Prognosis (what to expect long-term)
With prompt treatment, many patients improve, but GCA often requires long-term monitoring because relapses and vascular complications can occur. The most important early goal is preventing irreversible vision loss. Over time, care also focuses on tapering steroids safely, reducing relapse risk, and monitoring large-vessel disease.
Immediate treatment can protect vision.
Many patients improve quickly after steroids begin.
Long-term follow-up is still important because relapse or large-vessel complications can occur.
Understanding Giant Cell Arteritis: Complete Disease Explanation
Giant cell arteritis happens when immune-driven inflammation attacks the artery wall, especially in arteries containing elastic tissue. This causes thickening and narrowing of the vessel lumen, which can reduce blood flow to the eye, scalp, jaw, brain, or large arteries. A complete evaluation often looks beyond headache alone because some patients have large-vessel disease without classic temple symptoms.
What happens at the vessel level?
In GCA, inflammatory cells damage the artery wall and contribute to swelling, narrowing, and sometimes occlusion. This helps explain why the disease can cause ischemic symptoms such as jaw claudication or vision loss.
Immune vessel inflammation → artery narrowing → reduced blood flow → headache, jaw pain, visual risk, and vascular complications.
GCA vs polymyalgia rheumatica
Giant cell arteritis and polymyalgia rheumatica are closely linked inflammatory conditions and may occur together. PMR usually causes shoulder and hip girdle stiffness, while GCA is a vasculitis that threatens blood vessels and can endanger vision.
PMR symptoms may help raise suspicion for GCA in the right clinical setting.
GCA requires urgent attention because of the risk of irreversible vision loss.
Diagnosis: exam, labs, imaging
GCA is diagnosed using symptoms, physical exam, inflammatory markers, and confirmatory testing such as temporal artery ultrasound, biopsy, or imaging of large vessels. Doctors commonly check ESR, CRP, CBC, temporal artery findings, and may involve ophthalmology urgently when visual symptoms are present.
Tests often ordered during initial evaluation
Tests help support the diagnosis, assess inflammation, and identify vessel involvement.
- Inflammation markers such as ESR and CRP.
- Complete blood count, including anemia assessment.
- Temporal artery ultrasound or temporal artery biopsy.
- CT, MRI, PET, or other vascular imaging when large-vessel disease is suspected.
Treatment: urgent control + disease management
Effective giant cell arteritis treatment begins immediately because the first priority is protecting vision and limiting ischemic damage. High-dose corticosteroids are the main urgent treatment, and some patients may also receive tocilizumab or other steroid-sparing therapy depending on relapse risk and disease course.
1) Urgent control (protecting vision)
Suspected GCA with vision symptoms is a medical emergency. Steroid treatment is often started before biopsy confirmation to reduce the risk of permanent blindness. Patients with visual loss or major visual symptoms may need high-dose IV glucocorticoids rather than oral treatment alone.
2) Disease control (preventing relapse and complications)
After urgent control, long-term management focuses on gradual steroid tapering, relapse prevention, and monitoring for large-vessel complications. Tocilizumab is one option used in some patients to reduce steroid exposure and improve long-term disease control.
3) Lifestyle strategies that support treatment
- Report any new visual symptom, jaw pain, or sudden headache change immediately.
- Keep close follow-up during steroid taper because relapses can occur.
- Monitor blood pressure, bone health, and steroid side effects during treatment.
- Coordinate care with rheumatology and ophthalmology when eye symptoms are present.
Treatment targets (vision and vessel protection)
In GCA, treatment targets focus first on preventing vision loss and controlling vessel inflammation. Over time, clinicians also track relapse, large-vessel involvement, inflammatory markers, and steroid-related toxicity.
| Target area | What your clinician tracks | What “on target” can look like |
|---|---|---|
| Vision safety | Blurred vision, double vision, visual loss, eye symptoms | No new visual ischemic events |
| Vessel inflammation | Headache, jaw pain, ESR/CRP, artery tenderness | Reduced symptoms and lower inflammatory activity |
| Long-term control | Relapse, steroid dose, large-vessel monitoring | Stable disease with safer tapering |
Case Study 1 (Example)
Older patient developed severe headache, scalp tenderness, and vision disturbances, especially while chewing. Evaluation suggested giant cell arteritis rather than migraine- headache or sinus-related pain.
GCA vs migraine or tension headache (quick table)
GCA can sometimes be mistaken for a headache disorder, but it is different because it reflects inflamed blood vessels and can threaten vision. Jaw claudication, scalp tenderness, age over 50, elevated inflammatory markers, and visual symptoms are important clues that this is not a routine headache pattern.
| Feature | Giant cell arteritis (GCA) | Migraine / tension headache |
|---|---|---|
| Typical age | Usually over age 50 | Can occur at many ages |
| Temple tenderness | Common and may be focal | Not a defining vascular sign |
| Jaw pain with chewing | Important warning feature | Not typical |
| Vision threat | Can cause sudden permanent loss | Usually does not threaten blood flow to the eye |
When to seek urgent care
- New blurred vision, double vision, partial vision loss, or sudden blindness.
- New headache after age 50 with temple tenderness or jaw claudication.
- Scalp tenderness with systemic symptoms and concern for temporal arteritis.
- Sudden major worsening, neurologic symptoms, or symptoms suggesting stroke or severe vascular ischemia.
Call Now for Giant Cell Arteritis Care
⭐ Google Rating: 4.7/5 (184 reviews) • Insurance accepted: Most major plans (verify with office).
Patient testimonial: “My new temple headache and jaw pain were getting worse. The team acted quickly, explained the urgency, and helped me start treatment fast.”
Call Now: (352) 717-0603 Request AppointmentClinic Address
Rheumatology Care Associates PLLC (RCA)
2611 S US Hwy 27, Clermont, FL 34711
Email: info@rheumatologycareassociates.com
Office hours: Mon 8:30AM–5:00PM; Tue 8:30AM–5:00PM; Wed 8:00AM–3:30PM; Thu 8:30AM–5:00PM; Fri 9:00AM–1:30PM.
Related conditions (internal links)
FAQ
Conclusion
Giant cell arteritis is a treatable but urgent vasculitis that can threaten vision if not recognized quickly. If you have a new headache after age 50, jaw pain with chewing, scalp tenderness, or visual symptoms, urgent rheumatology or emergency evaluation can be vision-saving.
Disclaimer: This article is for educational purposes and does not replace professional medical advice. Always seek urgent medical attention for possible visual symptoms or suspected giant cell arteritis.
© 2026 Rheumatology Care Associates. All rights reserved.