
Medically reviewed by Dr. Priya Prakash (Rheumatologist, board certified) | Last updated: March 20, 2026
What Is Osteoporosis? Symptoms, Causes, Diagnosis & Treatment
Osteoporosis is a disease in which bones become weak, less dense, and more likely to break. It is often called a silent disease because many people have no symptoms until a fracture happens. Early diagnosis and treatment can reduce fracture risk, protect mobility, and help preserve long-term bone health.
If you’re searching what is osteoporosis, the simplest answer is that osteoporosis is a bone-weakening condition that makes fractures more likely, especially in the spine, hip, and wrist. Many people do not realize they have it until they break a bone, lose height, develop back pain from a spinal fracture, or notice a more stooped posture over time. A rheumatologist or other clinician can help confirm the diagnosis and create an individualized osteoporosis treatment plan based on bone density testing, fracture risk, medical history, and long-term prevention goals.
Osteoporosis becomes more common with aging, especially after menopause, but it can also occur in men and in younger adults with major risk factors. Long-term corticosteroid use, low body weight, low calcium or vitamin D intake, smoking, inactivity, and certain medical conditions can all contribute. Because osteoporosis often develops quietly for years before the first fracture, early screening and risk assessment matter.
Table of Contents
- What Is Osteoporosis? Simple medical definition
- Osteoporosis at a glance
- Common osteoporosis patterns
- Osteoporosis symptoms (what it feels like)
- Causes & risk factors
- How osteoporosis is recognized
- Comorbidities & whole-body impact
- Prognosis (what to expect long-term)
- Understanding osteoporosis: complete disease explanation
- Osteoporosis vs osteopenia
- Diagnosis: exam, labs, testing
- Treatment: symptom relief + long-term disease control
- Treatment targets (bone density, fractures, function)
- Osteoporosis vs osteoarthritis (quick table)
- When to seek urgent care
- Downloadable osteoporosis symptom checklist
- Related conditions (internal links)
- FAQs
- Conclusion + next steps
What Is Osteoporosis? Simple Medical Definition
Osteoporosis is a skeletal disease characterized by low bone mass and structural deterioration of bone tissue, which increases the risk of fragility fractures. In short, clinically, what is osteoporosis? It is a condition in which bone strength is reduced enough that everyday falls, minor trauma, or even ordinary movements in severe cases can lead to fractures, especially in the spine, hip, and wrist.
Osteoporosis at a Glance
Silent bone loss Many people have no symptoms until a fracture occurs
Fracture risk Spine, hip, and wrist fractures are especially important
Bone density decline Low bone mineral density increases fragility risk
Screening matters Bone density testing can detect osteoporosis before a fracture happens
Prevention is possible Exercise, nutrition, and treatment can help protect bone strength
Osteoporosis often causes no pain until a bone breaks, which is why screening and risk assessment are so important.
Common Osteoporosis Patterns
Osteoporosis can appear in different clinical settings, which is one reason risk assessment is important. Some patients develop age-related or postmenopausal bone loss, while others have secondary osteoporosis related to medications, endocrine disorders, inflammatory disease, malabsorption, or prolonged immobility. Clinicians often think about osteoporosis by fracture history, bone density severity, and whether there is an underlying reversible cause.
Postmenopausal osteoporosis Bone loss increases after estrogen decline
Age-related osteoporosis Bone density falls with aging and frailty
Secondary osteoporosis Steroids, endocrine disease, or other medical causes contribute
Fracture-predominant osteoporosis Disease is first recognized after a spine, hip, or wrist fracture
Screen-detected osteoporosis Low bone density is found before any major fracture happens
Osteoporosis symptoms (what it feels like)
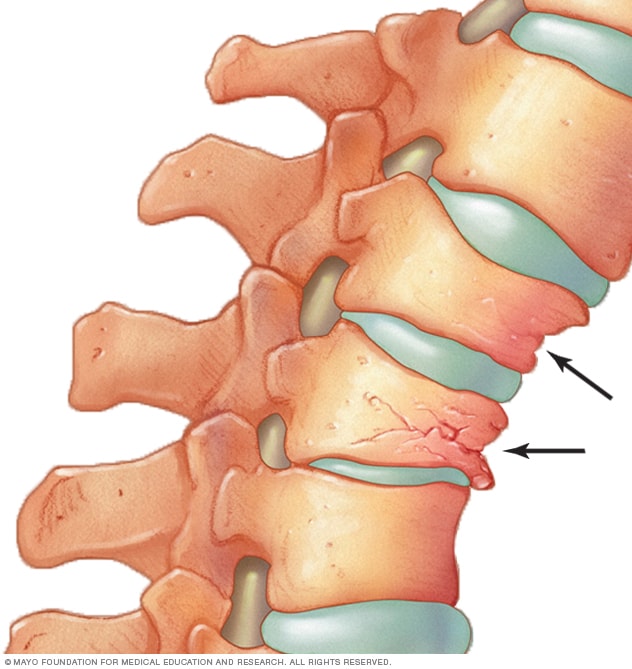
Typical osteoporosis symptoms are often absent until a fracture occurs. Many patients feel completely well until they develop a fragility fracture, but some later notice back pain, loss of height, or a stooped posture after vertebral compression fractures. Hip, spine, and wrist fractures can cause sudden pain, loss of independence, reduced mobility, and major changes in day-to-day function.
Spine • Hip • Wrist • Height loss • Posture • Balance • Fracture recovery • Mobility
Age, hormones
Steroids, low weight
Lower density
Fragile structure
Often silent
Fracture first
DXA testing
Fracture prevention
Wheel shows a simplified pathway: bone loss and weakened structure → higher fracture risk → evaluation and long-term fracture prevention.
Images for patient education
Spine fracture risk
Hip fracture concern

Bone density loss

Causes & risk factors
Osteoporosis develops when bone breakdown happens faster than the body can rebuild strong new bone. Aging, menopause, low sex-hormone states, poor calcium or vitamin D intake, lack of weight-bearing activity, smoking, alcohol excess, and chronic corticosteroid use are all important contributors. Secondary causes such as inflammatory disease, endocrine problems, kidney disease, malabsorption, and some cancer-related treatments can also increase risk.
- Older age and postmenopausal bone loss
- Prior fragility fracture or family history of hip fracture
- Long-term corticosteroid use
- Low body weight, poor nutrition, or low calcium/vitamin D intake
- Smoking, heavy alcohol use, and low physical activity
- Secondary medical causes that weaken bone
Evidence-based references (guidelines + high-quality sources)
General patient education: NIAMS. Clinical overview: Mayo Clinic. Diagnosis and treatment overview: Mayo Clinic.
How Osteoporosis Is Recognized
Osteoporosis is recognized through bone-density screening, fracture history, and overall fracture-risk assessment. Clinicians often look for age-related risk, prior fragility fractures, loss of height, posture changes, low body weight, corticosteroid exposure, and low bone mineral density on DXA scanning. The diagnosis may be made during routine screening or only after a spine, hip, or wrist fracture draws attention to underlying bone weakness.
Low bone density on DXA
Fragility fracture history
Height loss or posture change
Older age or postmenopausal status
Steroid exposure or major risk factors
High overall fracture-risk pattern
Comorbidities & whole-body impact
Osteoporosis can strongly affect long-term quality of life because fractures can reduce independence, mobility, posture, confidence, and daily activity. Back pain after vertebral fractures, fear of falling, frailty, hospitalization, deconditioning, and complications after hip fracture can all shape outcomes. Good care requires attention not only to bone density, but also to falls prevention, balance, muscle strength, nutrition, and medication safety.
- Vertebral fractures with back pain or height loss
- Hip fractures with major mobility impact
- Falls risk and reduced confidence walking
- Frailty, deconditioning, and loss of independence
- Posture changes such as kyphosis after spinal fractures
- Medication side effects and long-term adherence challenges
Prognosis (what to expect long-term)
The outlook for osteoporosis is often good when it is identified before major fractures occur and treated consistently. Even so, long-term outcomes depend on fracture history, fall risk, treatment adherence, age, and whether spine or hip fractures have already happened. The central goals are to prevent first and future fractures, preserve mobility, protect posture and independence, and reduce treatment-related complications.
Many fractures can be prevented with screening, lifestyle measures, and medication when needed.
The first fragility fracture is often a warning sign of higher future fracture risk.
Good control means stronger prevention, safer mobility, and better long-term independence.
Understanding Osteoporosis: Complete Disease Explanation
Osteoporosis occurs when the internal structure of bone becomes thinner and weaker over time. This happens because normal bone remodeling shifts toward more bone loss and less effective bone rebuilding. As a result, bones may look normal from the outside but become fragile enough to break more easily with falls, twisting, lifting, or even routine movement in severe disease.
What happens at the bone level?
Healthy bone is constantly renewed, but osteoporosis develops when that renewal process no longer keeps up with bone loss. Bone mineral density falls and the supporting internal microarchitecture becomes less strong. This is why osteoporosis is defined by fracture risk, not just by a lab value or one isolated symptom.
Bone remodeling imbalance → lower bone density and weaker structure → fragility fractures → need for screening, prevention, and long-term bone protection.
Osteoporosis vs osteopenia
Osteoporosis and osteopenia both involve lower-than-normal bone density, but they are not the same severity level. Osteopenia means bone density is below normal but not yet low enough to meet the diagnostic threshold for osteoporosis, while osteoporosis carries a clearly higher fracture risk. Distinguishing between them matters because medication decisions, follow-up intensity, and fracture-prevention planning may differ.
Osteopenia is lower bone density that has not yet reached osteoporosis-level severity.
Osteoporosis reflects greater structural weakness and higher fragility-fracture risk.
Correct classification helps guide screening intervals and treatment decisions.
Diagnosis: exam, labs, testing
Osteoporosis is diagnosed using fracture history, clinical risk assessment, and bone mineral density testing, usually with a DXA scan. Doctors may also review height loss, posture, prior fractures, balance, gait, diet, medications, and secondary causes that affect bone health. Blood work may be used to look for vitamin D deficiency or underlying conditions contributing to bone loss, especially when the pattern seems secondary rather than routine age-related disease.
Tests often ordered during initial evaluation
Tests help confirm the diagnosis, estimate fracture risk, and guide treatment safety.
- Bone mineral density testing with DXA scanning, usually at the spine and hip.
- Clinical history focused on fractures, falls, height loss, family history, menopause status, steroid use, and nutrition.
- Physical examination for posture, gait, balance, frailty, and loss of height.
- Blood tests such as calcium, vitamin D, kidney function, thyroid-related or other secondary-cause evaluation when needed.
- Spine imaging or other imaging when vertebral fracture is suspected because of pain, height loss, or posture change.
Treatment: symptom relief + long-term disease control
Effective osteoporosis treatment has two main goals: reduce fracture risk and protect long-term bone strength. Treatment may include weight-bearing exercise, fall prevention, adequate calcium and vitamin D intake, smoking cessation, alcohol moderation, and medications such as antiresorptive or bone-building therapy when fracture risk is high. Long-term care also includes repeat bone-density monitoring, medication review, and strategies to preserve strength, balance, and independence.
1) Symptom control (short-term relief)
Short-term care often focuses on pain control and restoring function after a fracture, especially when vertebral compression fractures cause back pain or loss of mobility. Supportive treatment may include activity adjustment, physical therapy, fall-risk assessment, and careful guidance on safe movement. Patients without fractures may not need symptom relief at all, but they still need prevention because silent bone loss can continue.
2) Long-term management (disease control and organ protection)
Long-term treatment may include calcium and vitamin D optimization, structured exercise, and prescription medication based on bone density and fracture history. The main goal is to reduce the chance of first and repeat fractures while preserving mobility and independence. Long-term care also includes repeat DXA testing, reassessment of fall risk, and review of medications or illnesses that continue to weaken bone.
3) Lifestyle strategies that support treatment
- Use regular weight-bearing and muscle-strengthening exercise as medically appropriate to support bone and balance.
- Reduce falls risk by addressing home hazards, poor balance, weak muscles, and vision issues.
- Maintain adequate calcium and vitamin D intake and review nutrition if body weight is low or intake is limited.
- Avoid smoking and keep alcohol use moderate because both can worsen bone health.
- Keep follow-up visits because fracture prevention depends on long-term monitoring, not one-time testing alone.
Treatment targets (bone density, fractures, function)
In osteoporosis, treatment targets focus on improving bone protection, lowering fracture risk, and preserving safe movement and independence. Clinicians track fractures, DXA trends, falls, posture, height loss, mobility, medication adherence, and risk factors that continue to weaken bone. Good control means more than a better scan number alone; it means fewer fractures, safer walking, and stronger long-term function.
| Target area | What your clinician tracks | What “on target” can look like |
|---|---|---|
| Bone protection | DXA results, calcium/vitamin D status, medication use, risk factors | Better long-term bone support and less ongoing bone loss |
| Function and falls | Balance, gait, muscle strength, height loss, mobility, home fall risks | Safer daily movement and lower falls risk |
| Fracture prevention | New fractures, vertebral symptoms, hip risk, treatment adherence, secondary causes | Fewer fractures and preserved independence over time |
Case Study 1 (Example)
Patient developed gradual height loss and later had a wrist fracture after a minor fall, followed by evaluation showing low bone density. Assessment suggested osteoporosis rather than routine age-related aches alone. A treatment plan focused on fracture prevention, bone-strength support, falls reduction, and long-term monitoring improved confidence and risk management over time.
Example: During high-risk bone loss, your clinician may use fracture-focused bone protection treatment based on DXA results, fracture history, overall risk, and safety factors.
Full details include fracture history, bone-density testing, risk-factor review, falls assessment, secondary-cause evaluation, and how treatment was adjusted over time using structured monitoring.
Osteoporosis vs osteoarthritis (quick comparison)
Osteoporosis and osteoarthritis both become more common with age, but they are very different conditions. Osteoporosis is a bone-fragility disease that raises fracture risk, while osteoarthritis is a joint-degeneration condition that mainly causes pain, stiffness, and mechanical joint symptoms. Distinguishing between them matters because osteoporosis may be silent until a fracture occurs, whereas osteoarthritis usually causes symptomatic joint complaints.
| Feature | Osteoporosis | Osteoarthritis |
|---|---|---|
| Main mechanism | Low bone density and weakened bone structure | Joint cartilage wear and structural joint change |
| Main problem | Fragility-fracture risk | Joint pain, stiffness, and function loss |
| Symptoms early on | Often none until fracture occurs | Often clear joint symptoms with use |
| Typical testing | DXA scan, fracture-risk assessment | Clinical exam and joint imaging when needed |
| Treatment focus | Fracture prevention and bone-strength protection | Pain relief, joint function, and mobility support |
When to seek urgent care
- Sudden severe back pain, especially after bending, lifting, or a minor fall.
- Hip pain, inability to bear weight, or loss of mobility after a fall or injury.
- Wrist, arm, or leg deformity or severe pain suggesting a fracture.
- Rapid decline in walking ability, repeated falls, or symptoms suggesting a new fragility fracture.
Call Now for Osteoporosis Care
⭐ Google Rating: 4.7/5 (184 reviews) • Insurance accepted: Most major plans (verify with office).
Patient testimonial: “I didn’t know my bones were weak until I fractured my wrist after a small fall. The team explained osteoporosis clearly and helped me understand how to prevent the next fracture.”
Call Now: (352) 717-0603 Request AppointmentClinic Address
Rheumatology Care Associates PLLC (RCA)
2611 S US Hwy 27, Clermont, FL 34711
Email: info@rheumatologycareassociates.com
Office hours: Mon 8:30AM–5:00PM; Tue 8:30AM–5:00PM; Wed 8:00AM–3:30PM; Thu 8:30AM–5:00PM; Fri 9:00AM–1:30PM.
Related conditions (internal links)
FAQ
Conclusion
Osteoporosis is a common but often silent disease that weakens bones and increases fracture risk over time. If you have risk factors such as menopause, steroid use, height loss, prior low-trauma fracture, or a family history of hip fracture, a medical evaluation can help confirm the diagnosis and build the right long-term bone-protection plan.
Disclaimer: This article is for educational purposes and does not replace professional medical advice. Always seek prompt care for suspected fracture, sudden severe back pain, hip pain after a fall, or loss of mobility.
© 2026 Rheumatology Care Associates. All rights reserved.