Medically reviewed by Dr. Priya Prakash (Rheumatologist, board certified) | Last updated: March 20, 2026
What Is Systemic Sclerosis (SSc)? Symptoms, Causes, Diagnosis & Treatment
Systemic sclerosis (SSc), also called systemic scleroderma, is a chronic autoimmune disease that causes abnormal blood-vessel dysfunction and excess scar-like tissue formation. This can lead to tight, thickened skin and may also affect the lungs, digestive tract, heart, kidneys, and other organs. Early diagnosis and regular organ screening are important because serious complications may develop even when early symptoms seem limited.
If you’re searching what is systemic sclerosis or what is scleroderma, the simplest answer is that SSc is a systemic autoimmune disease involving fibrosis, vascular injury, and immune dysfunction. Many patients first notice Raynaud’s phenomenon, puffy fingers, heartburn, skin tightening, or hand stiffness before the full pattern becomes obvious. A rheumatologist can help confirm the diagnosis and create an individualized systemic sclerosis treatment plan based on whether the disease is limited or diffuse, which organs are involved, and how active the vascular and fibrotic complications are.
sclerosis
Systemic sclerosis is not the same as localized scleroderma because SSc can affect internal organs as well as the skin. The two major clinical subsets are limited cutaneous systemic sclerosis and diffuse cutaneous systemic sclerosis, which differ in skin extent and risk profile. Because early symptoms can overlap with Raynaud’s phenomenon, reflux disease, inflammatory arthritis, or other connective tissue disorders, getting the diagnosis right matters.
Table of Contents
- What Is Systemic Sclerosis? Simple medical definition
- Systemic sclerosis at a glance
- Common systemic sclerosis patterns
- Systemic sclerosis symptoms (what it feels like)
- Causes & risk factors
- How systemic sclerosis is recognized
- Comorbidities & whole-body impact
- Prognosis (what to expect long-term)
- Understanding systemic sclerosis: complete disease explanation
- Limited vs diffuse systemic sclerosis
- Diagnosis: exam, labs, testing
- Treatment: symptom relief + long-term organ protection
- Treatment targets (vascular control, fibrosis, organ safety)
- Systemic sclerosis vs localized scleroderma (quick table)
- When to seek urgent care
- Downloadable systemic sclerosis symptom checklist
- Related conditions (internal links)
- FAQs
- Conclusion + next steps
What Is Systemic Sclerosis? Simple Medical Definition
Systemic sclerosis (SSc) is a chronic systemic autoimmune connective tissue disease characterized by microvascular injury, immune dysregulation, and progressive fibrosis of the skin and internal organs. In short, clinically, what is systemic sclerosis? It is a multisystem rheumatic disease in which abnormal collagen deposition and blood-vessel dysfunction lead to skin thickening, Raynaud’s phenomenon, and potential involvement of the lungs, gastrointestinal tract, heart, kidneys, and other organs.
Systemic Sclerosis at a Glance
Raynaud’s is common Many patients develop color change in fingers before other features appear
Skin tightening Fingers, hands, face, and other areas can become tight or thickened
Internal organ risk Lungs, GI tract, heart, and kidneys may be affected
Limited or diffuse forms Skin distribution helps define disease subset and risk pattern
Needs regular screening Serious organ complications may develop quietly
Systemic sclerosis is more than a skin condition. It is a vascular and fibrotic systemic disease that requires ongoing surveillance.
Common Systemic Sclerosis Patterns
Systemic sclerosis is often grouped by the extent of skin involvement and the pattern of internal-organ risk. Some patients have limited cutaneous disease with slower skin progression and long-standing Raynaud’s, while others have diffuse disease with more widespread skin thickening and faster internal-organ risk. Clinicians also think about systemic sclerosis by which complications dominate, such as interstitial lung disease, pulmonary hypertension, gastrointestinal involvement, digital ulcers, or renal crisis risk.
Limited cutaneous SSc Skin involvement usually stays distal, often with long-standing Raynaud’s
Diffuse cutaneous SSc More widespread skin involvement with higher early internal-organ risk
Vascular-dominant SSc Raynaud’s, digital ulcers, and pulmonary hypertension stand out
Fibrotic-organ SSc Lungs, skin, or GI tract show more prominent fibrosis-related disease
Overlap SSc Features of myositis, rheumatoid arthritis, or other connective tissue disease also appear
Systemic sclerosis symptoms (what it feels like)
Typical systemic sclerosis symptoms include Raynaud’s phenomenon, puffy or swollen fingers, skin tightness, reflux, and hand stiffness. Many patients notice fingers turning white, blue, or red in the cold, along with trouble bending the hands, digital ulcers, heartburn, bloating, constipation, cough, or shortness of breath. Some people also develop telangiectasias, calcinosis, joint pain, muscle weakness, hoarseness, swallowing problems, or reduced exercise tolerance depending on which organs are involved.
Fingers • Hands • Skin • Face • Esophagus • Stomach • Lungs • Heart • Kidneys • Blood vessels
Autoimmunity
Vascular injury
Excess collagen
Tissue scarring
Raynaud’s, skin
GI, lung signs
Subset, organs
Monitoring plan
Wheel shows a simplified pathway: vascular injury and immune dysfunction → fibrosis and organ effects → symptom pattern and long-term monitoring.
Images for patient education
Raynaud’s and fingers
Skin tightening
Internal organ involvement
Causes & risk factors
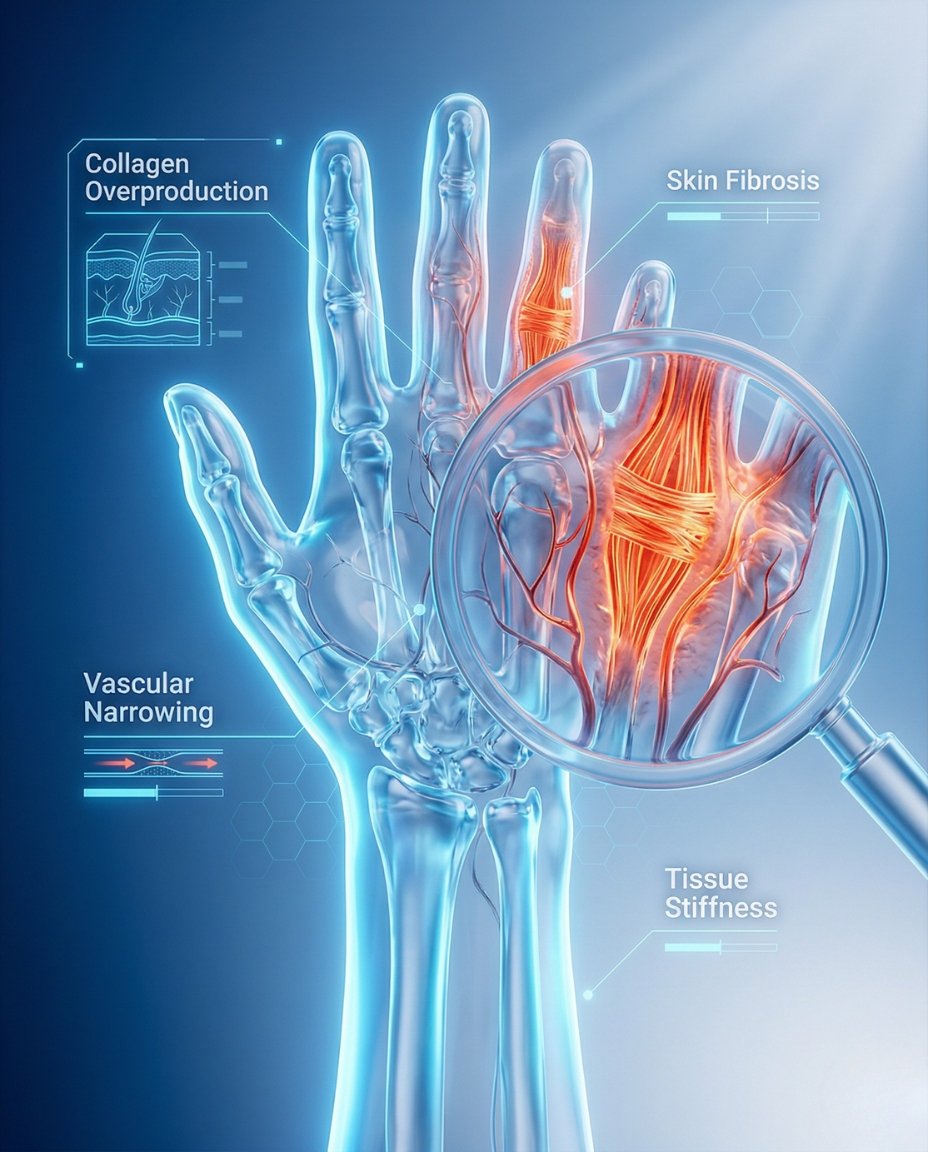
The exact cause of systemic sclerosis is not fully understood, but it involves a combination of immune dysregulation, blood-vessel injury, and abnormal fibroblast activation that produces excess collagen. Genetics and environmental factors may contribute, but the disease pattern reflects an abnormal healing and scarring response rather than simple inflammation alone. Women are affected more often than men, and different autoantibody patterns are linked to different complication risks.
- Autoimmune and vascular dysfunction
- Excess collagen production and fibrosis
- Raynaud’s phenomenon as a frequent early clue
- Different autoantibodies linked to different risk profiles
- Greater prevalence in women
- Internal-organ risk that depends on disease subset and antibody pattern
Evidence-based references (guidelines + high-quality sources)
General patient education: RheumInfo. Clinical overview: NIAMS. Professional review: NIH/NCBI StatPearls.
How Systemic Sclerosis Is Recognized
Systemic sclerosis is recognized through the pattern of Raynaud’s phenomenon, skin changes, vascular findings, autoantibodies, and evidence of internal-organ involvement. Specialists often look for puffy fingers, skin thickening, abnormal nailfold capillaries, reflux, shortness of breath, digital ulcers, or characteristic hand and facial changes. The diagnosis depends not only on skin findings, but also on understanding the wider vascular and organ pattern of the disease.
Raynaud’s phenomenon
Puffy fingers or skin thickening
Digital ulcers, telangiectasias, or calcinosis
Abnormal nailfold capillaries
SSc-related autoantibodies in many patients
GI, lung, heart, or kidney involvement in the right clinical pattern
Comorbidities & whole-body impact
Systemic sclerosis can affect many daily functions because it is both a vascular and fibrotic disease. Hand disability, reflux, swallowing problems, malnutrition risk, reduced exercise tolerance, lung disease, pulmonary hypertension, mood burden, and chronic pain can all affect quality of life. Some complications, such as scleroderma renal crisis, pulmonary arterial hypertension, and interstitial lung disease, are especially important because they can be life-threatening without early detection.
- Digital ulcers and hand dysfunction
- Severe reflux, dysmotility, bloating, or swallowing difficulty
- Interstitial lung disease
- Pulmonary arterial hypertension
- Scleroderma renal crisis risk in selected patients
- Cardiac involvement, malnutrition risk, and reduced quality of life
Prognosis (what to expect long-term)
The long-term outlook in systemic sclerosis depends heavily on the extent of internal-organ involvement. Limited disease may progress slowly, while diffuse disease or major lung, heart, pulmonary vascular, or kidney complications can change the risk profile substantially. The central goals are early recognition, regular screening, complication prevention, and treatment targeted to the organs most at risk.
Skin findings are only one part of prognosis.
Lung, pulmonary vascular, cardiac, and kidney complications are major drivers of long-term outcomes.
Good monitoring can detect important complications earlier and improve care decisions.
Understanding Systemic Sclerosis: Complete Disease Explanation
Systemic sclerosis develops when immune dysfunction, blood-vessel injury, and fibroblast overactivity combine to produce abnormal scarring. The skin becomes thickened and tight because excess collagen builds up, and similar processes can affect internal organs. Blood-vessel dysfunction is also central, which is why Raynaud’s, digital ischemia, and pulmonary vascular disease are such important parts of the illness.
What happens in the body?
The disease process begins with vascular injury and abnormal immune signaling, then drives fibroblasts to make too much collagen. This creates fibrosis in the skin and organs, while the damaged microvasculature contributes to tissue ischemia and poor repair. Together, these changes explain the combination of Raynaud’s phenomenon, skin tightening, ulcers, reflux, lung disease, and other organ complications.
Vascular injury and immune activation → fibroblast overactivity → excess collagen and fibrosis → skin changes plus internal-organ complications.
Limited vs diffuse systemic sclerosis
Limited and diffuse systemic sclerosis are both forms of the same disease, but they differ in skin distribution and complication patterns. Limited cutaneous disease usually affects the hands, lower arms, lower legs, and face, while diffuse cutaneous disease extends more proximally and often carries higher early internal-organ risk. This distinction matters because it helps guide screening intensity, prognosis discussion, and the urgency of monitoring for complications such as renal crisis or lung disease.
Limited SSc often has a longer vascular phase and may later develop pulmonary hypertension.
Diffuse SSc often has faster skin progression and higher early risk of internal-organ complications.
Correct subtype recognition helps guide surveillance and treatment priorities.
Diagnosis: exam, labs, testing
Systemic sclerosis is diagnosed using the overall clinical pattern, physical examination, autoantibody testing, and organ-assessment studies. Doctors may evaluate skin thickening, nailfold capillaroscopy findings, Raynaud’s pattern, autoantibodies such as ANA, anticentromere, anti-topoisomerase I, and anti-RNA polymerase III, along with pulmonary, cardiac, kidney, and GI testing. Because complications can be silent early on, diagnosis and follow-up also depend on routine surveillance even after the disease is identified.
Tests often ordered during initial evaluation
Tests help confirm the diagnosis, identify the disease subset, and screen for organ involvement.
- Detailed history of Raynaud’s phenomenon, reflux, skin tightness, ulcers, breathing symptoms, and swelling of the hands.
- Physical exam focusing on skin thickening, hand changes, telangiectasias, calcinosis, digital ulcers, and blood pressure.
- Blood tests including ANA and SSc-related autoantibodies such as anticentromere, anti-topoisomerase I, and anti-RNA polymerase III.
- Nailfold capillaroscopy to look for microvascular abnormalities.
- Pulmonary function tests, echocardiography, and often chest imaging to screen for interstitial lung disease or pulmonary hypertension.
- Kidney function tests, urinalysis, and blood pressure monitoring to assess renal risk.
Treatment: symptom relief + long-term organ protection
Effective systemic sclerosis treatment has two main goals: control complications and protect organ function. There is no single treatment that cures all forms of SSc, so care is usually organ-specific and complication-focused. Common management areas include Raynaud’s control, ulcer prevention, reflux treatment, immunomodulatory therapy for lung or skin disease in selected cases, and close monitoring for kidney, heart, and pulmonary vascular complications.
1) Symptom control (vascular and daily-function relief)
Raynaud’s and digital ischemia are often treated with warming strategies, avoidance of cold and nicotine, and blood-vessel relaxing medications such as calcium channel blockers. Reflux, swallowing problems, bowel symptoms, pain, and stiffness also need targeted supportive treatment. Hand therapy, skin care, and ulcer prevention may improve daily comfort and function.
2) Long-term management (organ-specific protection)
Long-term treatment depends on the organ systems involved and may include immunosuppressive therapy for interstitial lung disease or inflammatory overlap features, pulmonary hypertension treatment, ACE inhibitors for renal crisis situations, and structured monitoring plans. The treatment strategy is built around complication prevention and early intervention rather than one universal medication approach. This is why regular follow-up with rheumatology and other specialists is so important.
3) Lifestyle strategies that support treatment
- Protect hands and body from cold exposure to reduce Raynaud’s attacks and digital injury.
- Avoid smoking and nicotine because they worsen blood-vessel constriction.
- Seek prompt evaluation for increasing shortness of breath, severe reflux, blackened fingertips, or rising blood pressure.
- Keep scheduled organ-screening appointments even when symptoms seem stable.
- Use hand stretching, therapy, and skin care strategies when tightness limits function.
Treatment targets (vascular control, fibrosis, organ safety)
In systemic sclerosis, treatment targets focus on reducing vascular injury, protecting organs, preserving function, and detecting complications early. Clinicians track Raynaud’s frequency, skin progression, lung and heart testing, kidney health, GI symptoms, ulcers, and the patient’s ability to eat, breathe, and use the hands effectively. Good control means more than stable skin alone; it means safer lungs, circulation, kidneys, and long-term quality of life.
| Target area | What your clinician tracks | What “on target” can look like |
|---|---|---|
| Vascular symptoms | Raynaud’s attacks, digital ulcers, ischemic pain, nailfold changes | Fewer attacks and better fingertip protection |
| Fibrosis and function | Skin score, hand movement, reflux, swallowing, exercise tolerance | Stable skin and improved daily function |
| Organ safety | Lungs, pulmonary pressure, kidneys, heart, nutrition, blood pressure | Protected organ function and early complication detection |
Case Study 1 (Example)
Patient developed skin tightening over the fingers and face along with difficulty swallowing and cold sensitivity. Evaluation suggested systemic sclerosis rather than skin- thickening due to external causes or simple aging.
Systemic sclerosis vs localized scleroderma (quick comparison)
Systemic sclerosis and localized scleroderma are not the same condition. Localized scleroderma mainly affects the skin and tissues directly under it, while systemic sclerosis can also damage internal organs and blood vessels. Distinguishing between them is essential because the monitoring and long-term risks are very different.
| Feature | Systemic sclerosis | Localized scleroderma |
|---|---|---|
| Blood-vessel involvement | Common and clinically important | Usually not a defining systemic feature |
| Internal organs | May affect lungs, GI tract, heart, kidneys | Typically not systemic |
| Raynaud’s phenomenon | Common | Not usually central |
| Skin pattern | Often hand, face, and body distribution based on subtype | Localized plaques or bands |
| Monitoring needs | Regular organ screening required | Mainly skin-focused follow-up |
When to seek urgent care
- Sudden severe headache, rising blood pressure, reduced urination, or other signs suggesting scleroderma renal crisis.
- New or worsening shortness of breath, chest pain, fainting, or rapidly declining exercise tolerance.
- Blackened fingertips, severe digital pain, or signs of tissue loss from ischemia.
- Severe swallowing problems, dehydration, or major unexplained weight loss.
Call Now for Systemic Sclerosis Care
⭐ Google Rating: 4.7/5 (184 reviews) • Insurance accepted: Most major plans (verify with office).
Patient testimonial: “I thought I only had bad circulation and reflux until the finger changes and skin tightening progressed. The team recognized systemic sclerosis early and helped me understand the organ monitoring I needed.”
Call Now: (352) 717-0603 Request AppointmentClinic Address
Rheumatology Care Associates PLLC (RCA)
2611 S US Hwy 27, Clermont, FL 34711
Email: info@rheumatologycareassociates.com
Office hours: Mon 8:30AM–5:00PM; Tue 8:30AM–5:00PM; Wed 8:00AM–3:30PM; Thu 8:30AM–5:00PM; Fri 9:00AM–1:30PM.
Related conditions (internal links)
FAQ
Conclusion
Systemic sclerosis is a complex autoimmune vascular-fibrotic disease that can affect the skin and many internal organs over time. If you have Raynaud’s phenomenon, puffy fingers, skin tightening, reflux, or unexplained breathing symptoms, a rheumatology evaluation can help confirm the diagnosis and start the right organ-protective monitoring and treatment plan.
Disclaimer: This article is for educational purposes and does not replace professional medical advice. Always seek prompt care for possible renal crisis, breathing symptoms, or severe digital ischemia.
© 2026 Rheumatology Care Associates. All rights reserved.