Medically reviewed by Dr. Priya Prakash (Rheumatologist, board certified) | Last updated: March 20, 2026
What Is Polymyalgia Rheumatica (PMR)? Symptoms, Causes, Diagnosis & Treatment
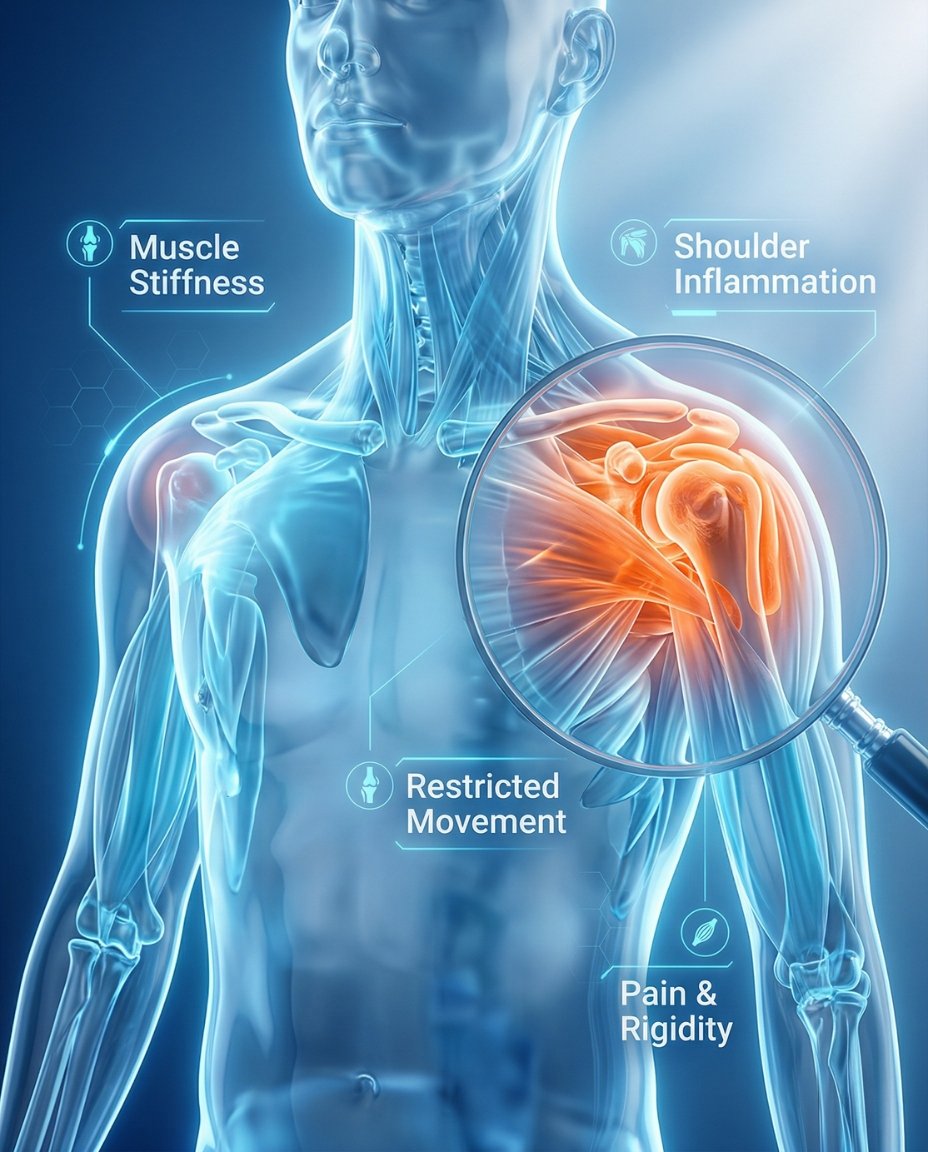
Polymyalgia rheumatica (PMR) is an inflammatory condition that causes pain and stiffness, mainly in the shoulders, upper arms, neck, hips, and thighs. Symptoms are usually much worse in the morning or after rest and can make basic movement feel difficult. Early diagnosis and treatment can reduce pain, restore mobility, and help monitor for related conditions such as giant cell arteritis.
If you’re searching what is polymyalgia rheumatica, the simplest answer is that PMR is an inflammatory disorder that causes prominent stiffness and aching in large muscle regions around the shoulders and hips. Many patients notice trouble getting out of bed, lifting the arms, getting dressed, rising from a chair, or walking comfortably after resting. A rheumatologist can confirm the diagnosis and create an individualized polymyalgia rheumatica treatment plan based on symptoms, exam findings, inflammatory markers, and response to treatment.
PMR almost always occurs in adults over age 50 and is closely linked with giant cell arteritis in some patients. Fatigue, low-grade fever, poor appetite, weight loss, and reduced energy can also occur alongside the stiffness. Because PMR can overlap with rheumatoid arthritis, myositis, hypothyroidism, infection, and other inflammatory conditions, getting the diagnosis right matters.
Table of Contents
- What Is Polymyalgia Rheumatica? Simple medical definition
- PMR at a glance
- Common PMR patterns
- Polymyalgia rheumatica symptoms (what it feels like)
- Causes & risk factors
- How PMR is recognized
- Comorbidities & whole-body impact
- Prognosis (what to expect long-term)
- Understanding PMR: complete disease explanation
- PMR vs giant cell arteritis
- Diagnosis: exam, labs, imaging
- Treatment: symptom relief + long-term monitoring
- Treatment targets (pain, stiffness, function)
- Polymyalgia rheumatica vs rheumatoid arthritis (quick table)
- When to seek urgent care
- Downloadable PMR symptom checklist
- Related conditions (internal links)
- FAQs
- Conclusion + next steps
What Is Polymyalgia Rheumatica? Simple Medical Definition
Polymyalgia rheumatica (PMR) is an inflammatory rheumatic condition that causes pain and marked stiffness, especially around the shoulders, neck, upper arms, hips, and thighs. In short, clinically, what is PMR? It is an inflammatory syndrome of older adults that typically causes profound morning stiffness, aching, reduced mobility, and elevated inflammatory markers, while often responding rapidly to low-dose corticosteroids.
PMR at a Glance
Shoulder and hip stiffness Usually affects both sides and is often severe in the morning
Age over 50 PMR almost always begins after age 50
Morning limitation Getting dressed, standing up, or raising the arms may be difficult
Inflammatory markers ESR and CRP are often elevated
Fast steroid response Many patients improve quickly after treatment starts
PMR usually causes stiffness more than true muscle weakness, even though patients often describe feeling weak because movement hurts.
Common PMR Patterns
Polymyalgia rheumatica often follows a recognizable pattern, but the exact presentation can still vary. Some patients mainly have shoulder and hip girdle stiffness, while others also develop constitutional symptoms such as fatigue, low appetite, or weight loss. Clinicians also consider whether PMR is isolated or whether there are features suggesting overlap with giant cell arteritis.
Classic bilateral PMR Shoulder and hip stiffness on both sides
Shoulder-dominant PMR Upper arm and neck discomfort stand out most
Systemic inflammatory PMR Fatigue, fever, or weight loss accompany stiffness
Relapsing PMR Symptoms improve, then return during tapering
PMR with GCA overlap Headache, jaw pain, scalp tenderness, or visual risk features appear
Polymyalgia rheumatica symptoms (what it feels like)
Typical polymyalgia rheumatica symptoms include aching and severe stiffness in the shoulders, neck, upper arms, hips, buttocks, or thighs. Symptoms are usually worse in the morning and after inactivity, and many patients describe difficulty turning in bed, getting up from a chair, climbing stairs, or lifting the arms overhead. PMR can also cause fatigue, low-grade fever, reduced appetite, poor sleep, and a general sense of being unwell.
Shoulders • Upper arms • Neck • Hips • Buttocks • Thighs • Morning mobility • Energy
Age over 50
Inflammatory tendency
Shoulder/hip girdles
Bursae and tissues
Pain, stiffness
Morning limitation
Confirm PMR
Treatment plan
Wheel shows a simplified pathway: inflammatory tissue irritation → pain and stiffness → evaluation and long-term monitoring.
Images for patient education
Shoulder stiffness
Hip girdle pain
Morning limitation

Causes & risk factors
The exact cause of PMR is not fully understood, but it is considered an inflammatory immune-mediated condition that occurs almost exclusively in older adults. Researchers think age-related immune changes, genetic factors, and environmental triggers may all play a role. PMR is not caused by normal aging alone, even though it becomes more common later in life.
- Age over 50, especially later adulthood
- Bilateral shoulder and hip aching with stiffness
- Morning stiffness lasting more than 45 minutes
- Elevated inflammatory markers such as ESR or CRP
- Rapid improvement after low-dose steroid treatment
- Need to watch for symptoms of giant cell arteritis
Evidence-based references (guidelines + high-quality sources)
General patient education: RheumInfo. Clinical overview: NIAMS. Professional review: NIH/NCBI StatPearls.
How PMR Is Recognized
PMR is recognized by its classic symptom pattern, age of onset, raised inflammatory markers, and exclusion of other causes of shoulder and hip girdle pain. Specialists often look for bilateral shoulder pain, morning stiffness longer than 45 minutes, hip involvement, difficulty with daily movement, elevated ESR or CRP, and a rapid response to low-dose prednisone. The diagnosis also depends on ruling out mimics such as rheumatoid arthritis, infection, thyroid disease, myositis, statin-related muscle symptoms, or other inflammatory conditions.
Age over 50
Bilateral shoulder pain and stiffness
Hip or thigh aching and stiffness
Morning stiffness often longer than 45 minutes
Elevated ESR or CRP
Rapid improvement with low-dose steroids
Comorbidities & whole-body impact
PMR can significantly affect sleep, mobility, independence, mood, and general quality of life when stiffness is severe. Some patients also have fatigue, low appetite, mild fever, weight loss, or reduced physical activity that leads to deconditioning over time. The most important related condition to monitor is giant cell arteritis, because new headache, scalp tenderness, jaw pain, or visual symptoms can signal an urgent vascular problem.
- Fatigue and reduced stamina
- Sleep disruption due to pain and stiffness
- Lower activity level and deconditioning
- Weight loss or poor appetite in some patients
- Relapse during steroid taper in some cases
- Giant cell arteritis overlap or later development
Prognosis (what to expect long-term)
PMR is usually very treatable, and many patients improve dramatically after starting corticosteroids. Even so, treatment often continues for many months, and some patients experience relapses as the steroid dose is reduced. The long-term goal is to control symptoms, taper medication safely, preserve function, and monitor carefully for giant cell arteritis and steroid-related side effects.
Many patients feel much better quickly after treatment begins.
Symptoms can return during steroid tapering in some cases.
Most people improve with careful follow-up and gradual dose adjustment over time.
Understanding PMR: Complete Disease Explanation
Polymyalgia rheumatica appears to involve inflammation in the tissues around the shoulders, hips, and nearby structures such as bursae and joint linings. This helps explain why patients often feel widespread stiffness and aching in the shoulder and hip girdles even though the muscles themselves are not usually the main damaged tissue. In daily life, the condition is often most obvious during the first movements of the morning or after sitting still for too long.
What happens at the body level?
In PMR, inflammatory activity affects movement around large proximal joints, which is why simple tasks can suddenly become difficult. Patients may say they feel weak, but on exam the problem is often pain-limited movement and stiffness rather than a true loss of muscle power. This distinction helps separate PMR from muscle diseases such as myositis.
Inflammatory tissue irritation around shoulders and hips → pain and stiffness → reduced morning mobility → improved movement after treatment and activity.
PMR vs giant cell arteritis
PMR and giant cell arteritis are closely linked inflammatory disorders and can occur together or appear at different times. PMR mainly causes severe stiffness and aching in the shoulders and hips, while giant cell arteritis affects blood vessels and can threaten vision. This connection is one of the most important safety issues in PMR care, because any new headache, jaw claudication, scalp tenderness, or visual change requires urgent attention.
PMR primarily affects comfort, movement, and function.
Giant cell arteritis can become a medical emergency because of vision loss risk.
Patients with PMR must be educated about GCA warning symptoms.
Diagnosis: exam, labs, imaging
PMR is diagnosed using the overall pattern of symptoms, age, inflammatory blood tests, physical exam findings, and exclusion of other conditions. Clinicians often check ESR and CRP, ask about the timing and distribution of stiffness, and look for whether the symptoms are symmetric and mainly proximal. Ultrasound or other imaging may be used in selected cases, especially when doctors need more support for the diagnosis or want to exclude another explanation.
Tests often ordered during initial evaluation
Tests help support the diagnosis, measure inflammation, and rule out mimics.
- Inflammation markers such as ESR and CRP.
- Basic blood tests to exclude other causes such as infection, anemia, thyroid disease, or muscle disease.
- Focused physical exam to assess shoulder and hip movement, stiffness pattern, and true muscle strength.
- Ultrasound, MRI, or other imaging in selected cases when the diagnosis is uncertain or a mimic is suspected.
Treatment: symptom relief + long-term monitoring
Effective polymyalgia rheumatica treatment has two main goals: relieve stiffness and pain quickly, and then taper medication safely while maintaining control. Low-dose corticosteroids, usually prednisone or prednisolone, are the standard initial treatment and often produce a dramatic improvement. Treatment then focuses on gradual dose reduction, monitoring for relapse, and limiting long-term steroid side effects.
1) Symptom control (short-term relief)
Most patients improve rapidly after starting a low-dose corticosteroid, which is one of the classic features of PMR. Improvement often begins within days, and sometimes even earlier, though full relief may still take longer. If symptoms do not improve as expected, clinicians may need to reconsider the diagnosis or look for another overlapping condition.
2) Long-term management (preventing relapse and treatment harm)
Once symptoms are controlled, the steroid dose is gradually tapered over many months. Some people can stop treatment within about a year, while others need longer treatment because symptoms return during tapering. Long-term care also includes watching for bone loss, blood sugar effects, blood pressure changes, infection risk, and other steroid-related complications.
3) Lifestyle strategies that support treatment
- Stay gently active and resume movement gradually as stiffness improves.
- Use physical therapy or guided exercise when function has dropped because of prolonged stiffness.
- Protect bone health during steroid use with appropriate calcium, vitamin D, and osteoporosis prevention when advised by your clinician.
- Report any new headache, scalp tenderness, jaw pain, or visual change immediately because these symptoms can suggest giant cell arteritis.
- Attend regular follow-up visits so medication tapering can be adjusted safely.
Treatment targets (pain, stiffness, function)
In PMR, treatment targets focus on lowering inflammation, reducing morning stiffness, restoring movement, and keeping symptoms controlled during steroid tapering. Clinicians track how easily the patient can get dressed, rise from a chair, lift the arms, turn in bed, and return to usual daily activity. Good control means more than lower pain alone; it means meaningful improvement in mobility and day-to-day function.
| Target area | What your clinician tracks | What “on target” can look like |
|---|---|---|
| Pain and stiffness | Morning duration, shoulder and hip symptoms, night discomfort | Much less stiffness and easier early-day movement |
| Function | Dressing, walking, rising from chair, lifting arms | Better mobility and more independence |
| Long-term control | Relapse during taper, ESR/CRP, steroid side effects, GCA symptoms | Stable symptoms with safer dose reduction |
Case Study 1 (Example)
Older patient developed sudden stiffness and pain in the shoulders and hips, especially in the morning. Evaluation suggested polymyalgia rheumatica rather than age-related- muscle stiffness or osteoarthritis alone.
Polymyalgia rheumatica vs rheumatoid arthritis (quick comparison)
PMR and rheumatoid arthritis can both cause pain and stiffness, but they usually present differently. PMR is more strongly centered on the shoulders, hips, and marked morning stiffness in older adults, while rheumatoid arthritis more often involves inflamed peripheral joints such as the hands and feet. PMR also tends to improve dramatically with low-dose steroids, whereas rheumatoid arthritis usually needs a different long-term disease-control strategy.
| Feature | Polymyalgia rheumatica (PMR) | Rheumatoid arthritis (RA) |
|---|---|---|
| Main pattern | Shoulder and hip girdle stiffness and aching | Inflammatory joint disease, often in hands and feet |
| Typical age | Usually over 50 | Can begin at many adult ages |
| Morning stiffness | Often severe and prolonged | Also prolonged, usually with clearer joint inflammation |
| True joint swelling | Usually limited or absent as the main feature | Common in active disease |
| Treatment response | Often rapid response to low-dose steroids | Usually requires DMARD-based long-term control |
When to seek urgent care
- New headache, scalp tenderness, jaw pain with chewing, or visual symptoms, because these may signal giant cell arteritis.
- Sudden vision change, double vision, or vision loss, which requires urgent emergency evaluation.
- High fever, marked illness, or symptoms suggesting infection rather than routine PMR.
- Rapid severe worsening or symptoms that no longer fit the usual PMR pattern.
Call Now for Polymyalgia Rheumatica Care
⭐ Google Rating: 4.7/5 (184 reviews) • Insurance accepted: Most major plans (verify with office).
Patient testimonial: “My morning stiffness was so bad I could barely get dressed. The team explained what PMR is and helped me feel better quickly.”
Call Now: (352) 717-0603 Request AppointmentClinic Address
Rheumatology Care Associates PLLC (RCA)
2611 S US Hwy 27, Clermont, FL 34711
Email: info@rheumatologycareassociates.com
Office hours: Mon 8:30AM–5:00PM; Tue 8:30AM–5:00PM; Wed 8:00AM–3:30PM; Thu 8:30AM–5:00PM; Fri 9:00AM–1:30PM.
Related conditions (internal links)
FAQ
Conclusion
Polymyalgia rheumatica is a treatable inflammatory condition that can strongly affect comfort, morning movement, sleep, and independence if not recognized early. If you have new severe morning shoulder and hip stiffness after age 50, especially with fatigue or raised inflammatory markers, a rheumatology evaluation can help clarify the diagnosis and next steps.
Disclaimer: This article is for educational purposes and does not replace professional medical advice. Always seek urgent medical care for possible giant cell arteritis symptoms such as visual change, new headache, or jaw pain with chewing.
© 2026 Rheumatology Care Associates. All rights reserved.