Medically reviewed by Dr. Priya Prakash (Rheumatologist, board certified) | Last updated: March 20, 2026
What Is Granulomatosis with Polyangiitis (GPA)? Symptoms, Causes, Diagnosis & Treatment
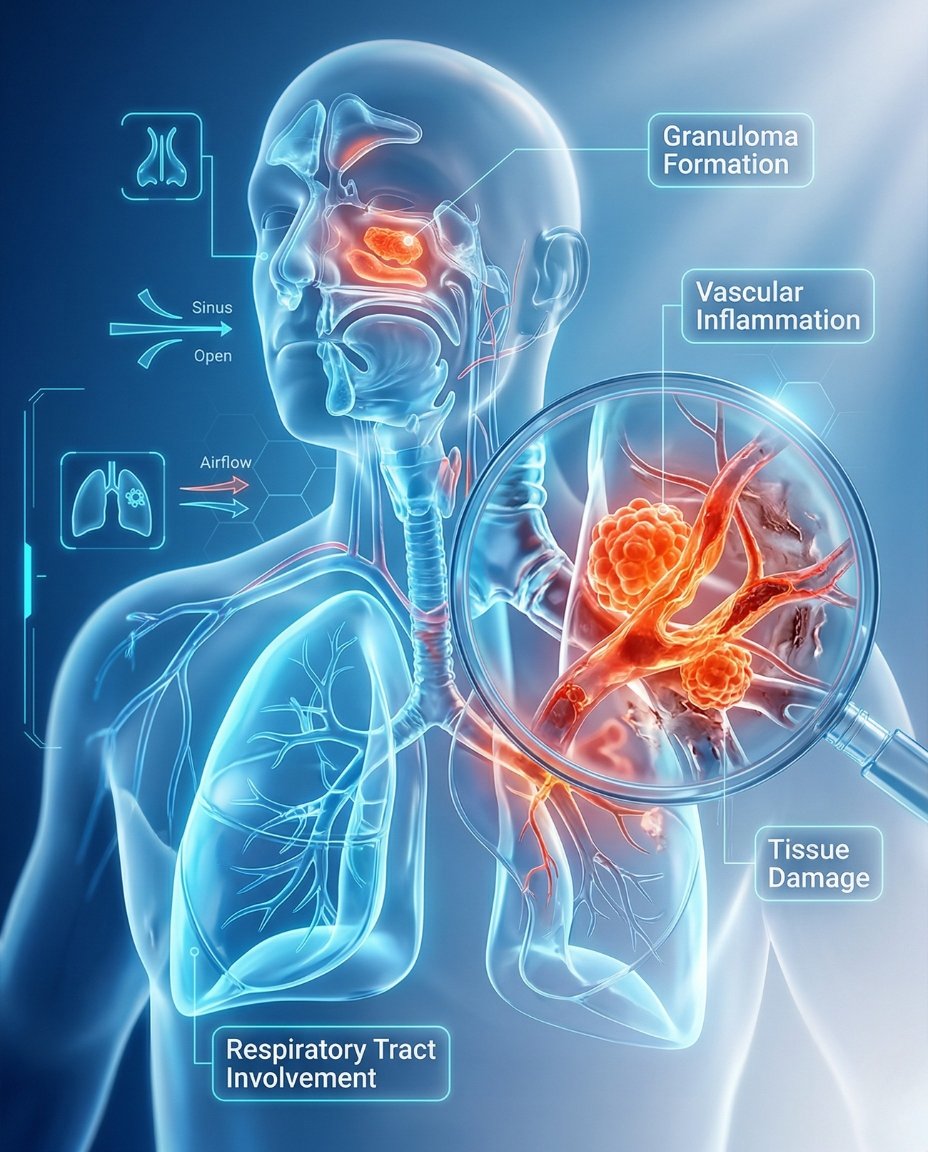
Granulomatosis with polyangiitis (GPA) is a rare autoimmune vasculitis that causes inflammation in small and medium blood vessels. It most commonly affects the nose, sinuses, ears, lungs, and kidneys, but it can involve almost any organ in the body. Early diagnosis and treatment are essential because GPA can progress quickly and lead to permanent organ damage if it is not treated promptly.
If you’re searching what is GPA, the simplest answer is that it is a form of vasculitis in which blood-vessel inflammation and granulomatous tissue injury reduce normal blood flow and damage surrounding tissues. Many patients first notice chronic sinus problems, nosebleeds, ear symptoms, cough, shortness of breath, fatigue, or kidney-related changes before the full disease pattern is recognized. A rheumatologist can help confirm the diagnosis and create an individualized GPA treatment plan based on organ involvement, disease severity, ANCA status, and whether the goal is remission induction or relapse prevention.
GPA was formerly called Wegener’s granulomatosis and belongs to the group of ANCA-associated vasculitides. Some people present with mainly ENT and lung symptoms, while others have rapidly progressive kidney disease, eye disease, skin vasculitis, or multisystem involvement. Because GPA can mimic chronic sinus infection, pneumonia, tuberculosis, cancer, kidney disease, or other vasculitides, getting the diagnosis right matters.
Table of Contents
- What Is GPA? Simple medical definition
- GPA at a glance
- Common GPA patterns
- GPA symptoms (what it feels like)
- Causes & risk factors
- How GPA is recognized
- Comorbidities & whole-body impact
- Prognosis (what to expect long-term)
- Understanding GPA: complete disease explanation
- GPA vs EGPA
- Diagnosis: exam, labs, testing
- Treatment: symptom relief + long-term disease control
- Treatment targets (vasculitis, remission, organ protection)
- GPA vs microscopic polyangiitis (quick table)
- When to seek urgent care
- Downloadable GPA symptom checklist
- Related conditions (internal links)
- FAQs
- Conclusion + next steps
What Is GPA? Simple Medical Definition
Granulomatosis with polyangiitis (GPA) is a rare ANCA-associated necrotizing vasculitis that primarily affects small and medium vessels and is characterized by granulomatous inflammation. In short, clinically, what is GPA? It is a systemic autoimmune vasculitis that most often targets the upper airways, lungs, and kidneys, but can also involve the eyes, skin, nerves, joints, and other organs.
GPA at a Glance
ENT symptoms common Chronic sinusitis, nosebleeds, ear symptoms, and nasal crusting are common clues
Lung involvement Cough, shortness of breath, lung nodules, or bleeding may occur
Kidney risk Kidney inflammation can develop silently and become severe quickly
ANCA-associated vasculitis PR3-ANCA is common, but not every case is the same
Can become organ-threatening Rapid treatment matters to prevent permanent damage
GPA is more than a sinus or lung disorder. It is a systemic vasculitis that can threaten kidney function, breathing, vision, and overall health.
Common GPA Patterns
GPA can present in a limited form or as widespread systemic disease. Some patients mainly have upper-airway and lung disease, while others also develop kidney inflammation, eye disease, skin lesions, joint pain, or nerve involvement. Clinicians often think about GPA by which organs are involved, whether the disease is organ-threatening, and whether the current goal is remission induction or maintenance after control is achieved.
ENT-dominant GPA Sinuses, nose, ears, and upper airway are most affected
Pulmonary GPA Cough, lung nodules, infiltrates, or bleeding dominate the picture
Renal GPA Kidney inflammation becomes a major driver of severity
Generalized GPA Multiple organs such as lungs, kidneys, eyes, skin, and nerves are involved
Relapsing GPA Disease returns after remission and needs long-term monitoring
GPA symptoms (what it feels like)
Typical GPA symptoms include chronic sinus congestion, nosebleeds, ear symptoms, cough, shortness of breath, fatigue, joint pain, and kidney abnormalities. Many patients notice persistent “sinus infection” symptoms that do not resolve, nasal crusting, hearing changes, chest symptoms, blood in sputum, unexplained fevers, or weight loss. Some people also develop eye inflammation, skin rash, purpura, nerve symptoms, swollen joints, or blood and protein in the urine as the disease progresses.
Nose • Sinuses • Ears • Lungs • Kidneys • Eyes • Skin • Nerves • Joints
ANCA pattern
Autoimmunity
Granulomas
Blood-vessel injury
ENT, lungs
Kidneys, eyes
Confirm GPA
Protect organs
Wheel shows a simplified pathway: ANCA-associated vasculitis and granulomatous inflammation → ENT, lung, kidney, and multisystem symptoms → organ-focused management.
Images for patient education
Sinus and nasal disease
Lung involvement
Kidney and systemic risk
Causes & risk factors
The exact cause of GPA is not fully understood, but it is an autoimmune vasculitis associated with abnormal immune activation and often ANCA antibodies, especially PR3-ANCA in many cases. The disease causes inflammation in blood vessels and granulomatous inflammation in tissues, which disrupts organ function and can lead to permanent damage if untreated. It is considered a rare disease, and its onset likely reflects a mix of immune susceptibility and environmental triggers rather than one single known cause.
- Autoimmune ANCA-associated vasculitis mechanism
- PR3-ANCA is common in many patients
- Granulomatous tissue inflammation plus vessel injury
- High risk of ENT, lung, and kidney involvement
- Rare disease that can worsen quickly
- Early treatment is critical to reduce permanent organ damage
Evidence-based references (guidelines + high-quality sources)
General patient education: RheumInfo. Clinical overview: Vasculitis Foundation. Professional review: NIH/NCBI StatPearls.
How GPA Is Recognized
GPA is recognized by the overall pattern of chronic upper-airway disease, lung findings, kidney abnormalities, positive ANCA in many patients, and supportive biopsy or imaging results. Specialists often suspect GPA when “sinus infections” keep recurring, nosebleeds or nasal crusting persist, cough or lung nodules appear, and urine testing shows blood or protein without another clear explanation. Diagnosis may require putting together ENT, pulmonary, kidney, laboratory, and pathology clues rather than relying on one single test.
Chronic sinusitis, nasal crusting, or nosebleeds
Ear symptoms or hearing changes
Lung nodules, cough, infiltrates, or coughing blood
Kidney inflammation with abnormal urine findings
PR3-ANCA or other ANCA support in many cases
Biopsy showing vasculitis or granulomatous inflammation when obtained
Comorbidities & whole-body impact
GPA can affect quality of life through both active vasculitis and the consequences of treatment. Chronic sinus disease, hearing problems, breathing symptoms, kidney impairment, fatigue, eye inflammation, nerve injury, relapse risk, and long-term steroid burden can all become major issues. Some complications, especially kidney failure, alveolar hemorrhage, and destructive ENT disease, can have lasting effects even after inflammation is brought under control.
- Chronic ENT damage including nasal and sinus complications
- Lung inflammation or bleeding risk
- Kidney inflammation and kidney-failure risk
- Eye inflammation that may threaten vision
- Skin, nerve, and joint involvement in some patients
- Relapse risk and medication side-effect burden
Prognosis (what to expect long-term)
The outlook for GPA has improved greatly with modern treatment, and remission is often achievable. However, the disease can still be severe, relapses are common, and long-term damage can occur if diagnosis or treatment is delayed. The most important goals are to induce remission quickly, protect organs, monitor for relapse, and minimize treatment toxicity over time.
Many patients can reach remission with prompt treatment.
Relapse monitoring remains important even after improvement.
Kidney, lung, and eye involvement strongly influence long-term risk.
Understanding GPA: Complete Disease Explanation
GPA combines blood-vessel inflammation with granulomatous tissue inflammation. This causes reduced blood flow and direct tissue injury, especially in the upper respiratory tract, lungs, and kidneys. That is why a patient may seem to have stubborn sinus disease at first, then later develop lung findings, blood in the urine, or other organ-threatening complications.
What happens in the body?
In GPA, the immune system activates inflammatory pathways that damage vessel walls and surrounding tissues. Granulomatous inflammation is especially important in the ENT and lung areas, while pauci-immune vasculitis often drives the kidney disease. Together, these changes explain why GPA can look like both a chronic destructive ENT condition and a systemic vasculitic illness at the same time.
ANCA-associated immune injury → vasculitis and granulomatous inflammation → ENT, lung, kidney, eye, skin, and nerve complications.
GPA vs EGPA
GPA and EGPA are both ANCA-associated vasculitides, but they have different hallmark patterns. GPA is more strongly linked to destructive ENT disease, lung nodules, and kidney vasculitis, while EGPA is closely associated with asthma, eosinophilia, sinus disease, and eosinophilic tissue injury. Distinguishing between them helps guide the diagnostic workup and long-term treatment approach.
GPA often presents with persistent ENT damage and renal vasculitis.
EGPA usually has asthma and marked eosinophilia as major clues.
Correct classification helps guide lab interpretation, biopsy strategy, and therapy planning.
Diagnosis: exam, labs, testing
GPA is diagnosed using the overall clinical pattern, ANCA testing, imaging, urine studies, kidney assessment, and biopsy when possible. Doctors may order CBC, inflammatory markers, creatinine, urinalysis, PR3-ANCA or MPO-ANCA testing, chest imaging, sinus imaging, and organ-specific evaluation depending on symptoms. Biopsy of affected tissue, such as kidney, nasal tissue, lung, or skin, can be very important when confirmation is needed and the site is safe to sample.
Tests often ordered during initial evaluation
Tests help confirm the diagnosis, define organ involvement, and rule out major mimics.
- Blood tests including CBC, ESR, CRP, kidney function, and ANCA testing.
- Urinalysis and urine protein assessment to look for kidney inflammation.
- Chest X-ray or CT scan for nodules, infiltrates, or bleeding.
- Sinus or ENT imaging when upper-airway disease is prominent.
- Biopsy of kidney, lung, nasal tissue, skin, or another affected organ when clinically appropriate.
- Eye, hearing, and nerve evaluation when those organs are involved.
Treatment: symptom relief + long-term disease control
Effective GPA treatment has two main goals: control active vasculitis quickly and prevent relapse over the long term. Severe or organ-threatening disease often requires remission-induction therapy with corticosteroids plus another potent immune-targeting treatment, while milder disease may be approached somewhat differently. Once remission is achieved, maintenance therapy and careful monitoring are essential because GPA commonly relapses.
1) Symptom control (short-term relief)
Corticosteroids are often used early to bring active inflammation down quickly. Supportive treatment also depends on the organs involved and may include airway care, oxygen support, kidney monitoring, or eye care when needed. In severe disease, rapid intervention is critical when there is kidney injury, lung bleeding, or vision-threatening inflammation.
2) Long-term management (remission induction and maintenance)
Long-term treatment often includes remission-induction therapy followed by maintenance treatment to reduce relapse risk. Depending on severity and response, clinicians may use agents such as rituximab, cyclophosphamide, methotrexate, azathioprine, mycophenolate, or other immunosuppressive strategies. The exact regimen depends on organ involvement, relapse history, kidney status, ANCA pattern, and medication safety factors.
3) Lifestyle strategies that support treatment
- Report coughing blood, new blood in urine, severe sinus destruction, eye pain, or vision changes urgently.
- Keep laboratory and urine monitoring appointments because kidney disease can worsen quietly.
- Follow airway, ENT, pulmonary, and nephrology recommendations when multiple organs are involved.
- Track relapses carefully, including sinus, lung, urine, and constitutional symptoms.
- Protect bone and infection risk during long-term corticosteroid or immunosuppressive therapy.
Treatment targets (vasculitis, remission, organ protection)
In GPA, treatment targets focus on stopping active vasculitis, protecting organs, reaching remission, and reducing relapse risk. Clinicians track ENT symptoms, lung findings, urine abnormalities, kidney function, ANCA context, imaging changes, and medication side effects over time. Good control means not only symptom improvement, but also prevention of silent kidney damage and serious relapse.
| Target area | What your clinician tracks | What “on target” can look like |
|---|---|---|
| Active vasculitis symptoms | Sinus disease, nosebleeds, cough, fatigue, fever, rash, joint symptoms | Less active inflammation and improved daily symptoms |
| Organ involvement | Lung imaging, urine findings, kidney function, eye symptoms, nerve changes | Stable or improving organ function |
| Remission and relapse prevention | Relapse pattern, maintenance therapy response, safety labs, steroid burden | Sustained remission with lower damage and safer long-term treatment |
Case Study 1 (Example)
Patient developed persistent sinus infections, nosebleeds, and fatigue along with breathing difficulty. Evaluation suggested granulomatosis with polyangiitis rather than chronic- sinusitis or common respiratory infection.
GPA vs microscopic polyangiitis (quick comparison)
GPA and microscopic polyangiitis are both ANCA-associated vasculitides, but they are not identical. GPA is more strongly associated with granulomatous ENT and lung disease, while microscopic polyangiitis more often presents with vasculitis affecting kidneys and lungs without the same granulomatous upper-airway pattern. This distinction matters because the clinical picture and biopsy clues can be different even when treatments overlap.
| Feature | GPA | Microscopic polyangiitis |
|---|---|---|
| ENT disease | Common and often prominent | Less typical as a dominant feature |
| Granulomatous inflammation | Characteristic feature | Not a defining pattern |
| Lungs | Nodules, infiltrates, bleeding can occur | Bleeding and vasculitic lung disease can occur |
| Kidneys | Commonly affected | Commonly affected |
| Overall pattern | ENT-lung-kidney pattern often stands out | Renal-pulmonary vasculitis pattern often stands out |
When to seek urgent care
- Coughing blood, severe shortness of breath, or suspected lung bleeding.
- Reduced urine, swelling, or signs of rapidly worsening kidney involvement.
- Eye pain, eye redness with vision change, or symptoms suggesting eye-threatening inflammation.
- Rapidly worsening weakness, severe systemic illness, or major bleeding symptoms.
Call Now for GPA Care
⭐ Google Rating: 4.7/5 (184 reviews) • Insurance accepted: Most major plans (verify with office).
Patient testimonial: “I thought I had nonstop sinus infections until the cough and abnormal labs showed something bigger was going on. The team recognized GPA and helped me start treatment quickly.”
Call Now: (352) 717-0603 Request AppointmentClinic Address
Rheumatology Care Associates PLLC (RCA)
2611 S US Hwy 27, Clermont, FL 34711
Email: info@rheumatologycareassociates.com
Office hours: Mon 8:30AM–5:00PM; Tue 8:30AM–5:00PM; Wed 8:00AM–3:30PM; Thu 8:30AM–5:00PM; Fri 9:00AM–1:30PM.
FAQ
Conclusion
GPA is a rare but treatable vasculitis that can damage the ENT tract, lungs, kidneys, and other organs if it is not recognized early. If you have persistent sinus disease, nosebleeds, cough, chest symptoms, abnormal urine, or other unexplained inflammatory symptoms, a rheumatology evaluation can help confirm the diagnosis and start the right organ-protective treatment plan.
Disclaimer: This article is for educational purposes and does not replace professional medical advice. Always seek prompt care for coughing blood, kidney symptoms, vision changes, or rapidly worsening illness.
© 2026 Rheumatology Care Associates. All rights reserved.