Medically reviewed by Dr. Priya Prakash (Rheumatologist, board certified) | Last updated: March 20, 2026
What Is Pseudogout? Symptoms, Causes, Diagnosis & Treatment
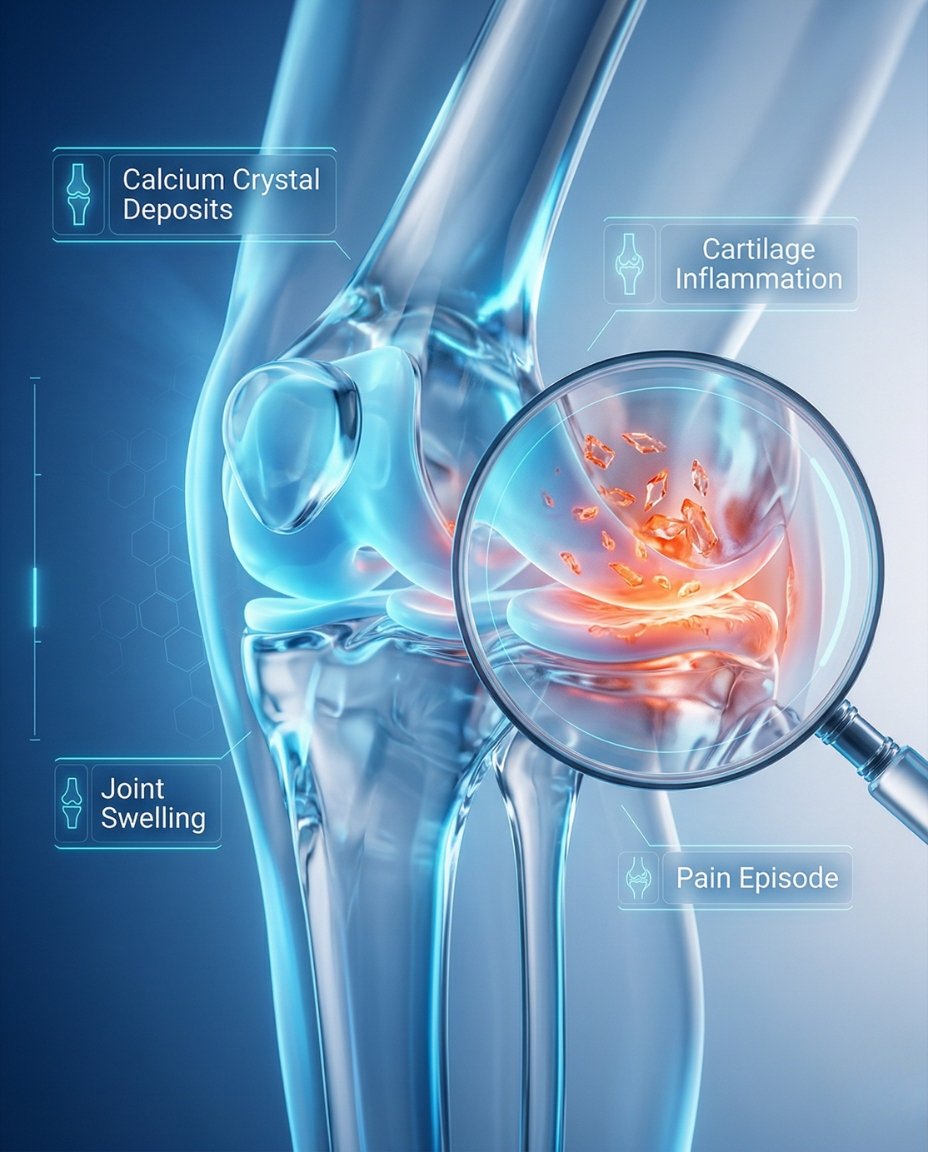
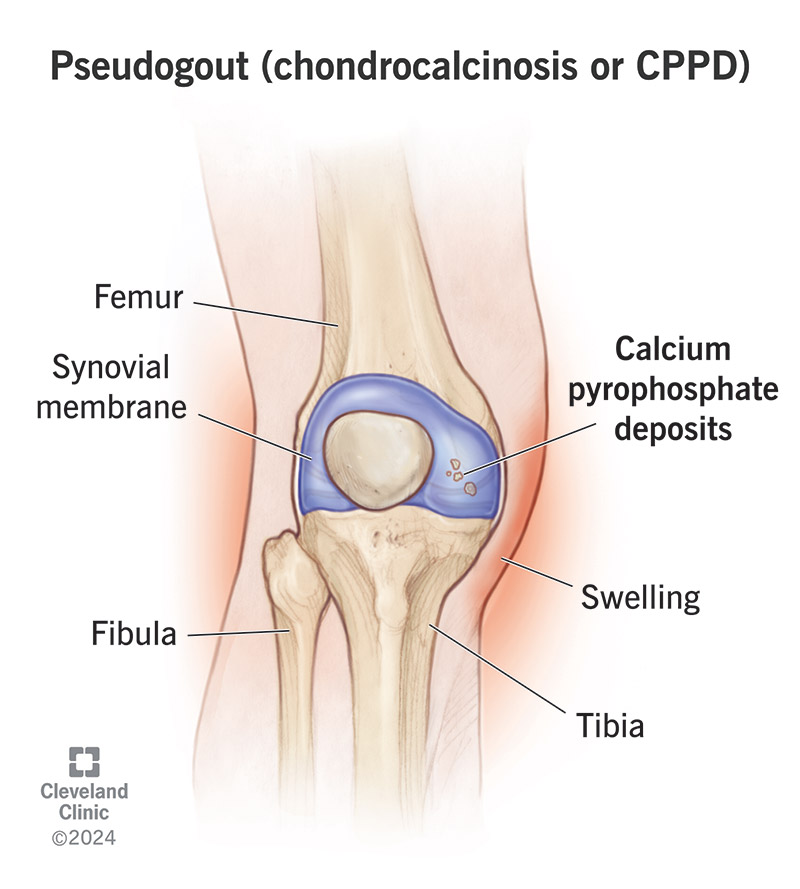
Pseudogout is a type of crystal arthritis caused by calcium pyrophosphate crystal buildup inside a joint. The medical term is calcium pyrophosphate deposition disease (CPPD), and the acute flare form is often called pseudogout because it can resemble gout. These crystal attacks can cause sudden severe pain, swelling, warmth, stiffness, and redness in one or more joints.
If you’re searching what is pseudogout, the simplest answer is that it is an inflammatory arthritis caused by calcium pyrophosphate crystals in the joint rather than uric acid crystals. During a flare, the immune system reacts to those crystals and the joint can become hot, swollen, red, and very painful over a short period of time. A rheumatologist can confirm the diagnosis and create an individualized pseudogout treatment plan based on the joint involved, severity of the attack, recurrence pattern, and whether there are underlying metabolic contributors.
Pseudogout most often affects older adults and commonly involves the knees, wrists, ankles, shoulders, elbows, or other large joints. Some patients have occasional isolated attacks, while others develop more chronic or recurrent inflammatory joint symptoms over time. Because pseudogout can look like gout, osteoarthritis, rheumatoid arthritis, or even a joint infection, getting the diagnosis right matters.
Table of Contents
- What Is Pseudogout? Simple medical definition
- Pseudogout at a glance
- Common CPPD patterns
- Pseudogout symptoms (what it feels like)
- Causes & risk factors
- How pseudogout is recognized
- Comorbidities & whole-body impact
- Prognosis (what to expect long-term)
- Understanding pseudogout: complete disease explanation
- Pseudogout vs gout
- Diagnosis: exam, labs, imaging
- Treatment: flare control + long-term management
- Treatment targets (pain, inflammation, recurrence)
- Pseudogout vs septic arthritis (quick table)
- When to seek urgent care
- Downloadable pseudogout symptom checklist
- Related conditions (internal links)
- FAQs
- Conclusion + next steps
What Is Pseudogout? Simple Medical Definition
Pseudogout is the acute inflammatory form of calcium pyrophosphate deposition disease (CPPD), a crystal arthropathy caused by calcium pyrophosphate crystal deposition in joints and surrounding tissues. In short, clinically, what is pseudogout? It is a crystal-triggered inflammatory arthritis in which calcium pyrophosphate crystals provoke a sudden immune response, causing joint pain, swelling, warmth, stiffness, and sometimes redness.
Pseudogout at a Glance
Sudden flare Symptoms often begin quickly rather than gradually
Hot swollen joint The joint may become red, warm, and very painful
Large joints common Knees and wrists are frequent sites
Older adults CPPD becomes more common with age
Looks like gout or infection Crystal attacks can mimic other urgent joint conditions
Pseudogout is not the same disease as gout, even though the attack pattern can feel very similar.
Common CPPD Patterns
Calcium pyrophosphate deposition disease can appear in more than one way. Some patients have sudden acute attacks called pseudogout, while others have chronic inflammatory symptoms, OA-like symptoms in unusual joints, or CPPD found on imaging without many symptoms. Clinicians often think about CPPD by flare pattern, chronicity, and whether the crystal disease is causing isolated attacks or ongoing joint trouble.
Acute pseudogout Sudden painful inflammatory flare in one or more joints
Recurrent CPPD Repeated flares over time
Chronic CPP inflammatory arthritis Ongoing inflammatory symptoms that may mimic RA
OA with CPPD Degenerative arthritis plus calcium crystal deposition
Asymptomatic chondrocalcinosis Crystal deposits seen on imaging without major symptoms
Pseudogout symptoms (what it feels like)
Typical pseudogout symptoms include sudden joint pain, swelling, warmth, redness, and stiffness. The joint may become difficult to move and can feel extremely tender even with light touch or motion. Flares can last for days or weeks, and while the knee is the classic site, the wrist, ankle, shoulder, elbow, and other large joints can also be involved.
Knees • Wrists • Ankles • Shoulders • Elbows • Hips • Large joints
Age, joint damage
Metabolic triggers
CPP crystals
Cartilage deposition
Pain, swelling
Hot joint flare
Joint fluid test
Treatment plan
Wheel shows a simplified pathway: calcium pyrophosphate crystals → joint inflammation → acute flare and long-term management.
Images for patient education
Hot swollen knee
Crystal inflammation

Wrist and ankle flare
Causes & risk factors
Pseudogout is caused by the deposition of calcium pyrophosphate crystals inside joints. Those crystals trigger inflammation when the immune system reacts to them, leading to an attack of acute crystal arthritis. Risk rises with age and may also be linked to previous joint damage, osteoarthritis, surgery or trauma to a joint, and certain metabolic conditions such as hyperparathyroidism, hemochromatosis, hypomagnesemia, or other mineral-balance disorders.
- Older age, especially later adulthood
- Prior joint damage, surgery, or osteoarthritis
- Sudden painful swelling in a large joint
- Calcium pyrophosphate crystals in joint fluid
- Chondrocalcinosis or calcification seen on imaging
- Possible associated metabolic disorders such as hemochromatosis or hyperparathyroidism
Evidence-based references (guidelines + high-quality sources)
General patient education: RheumInfo. Clinical overview: American College of Rheumatology. Professional review: NIH/NCBI StatPearls.
How Pseudogout Is Recognized
Pseudogout is recognized by the pattern of acute inflammatory joint attacks, supportive imaging findings, and ideally confirmation of calcium pyrophosphate crystals in the joint fluid. Specialists often look for a sudden hot swollen joint in an older adult, especially involving the knee or wrist, and consider whether X-rays show chondrocalcinosis. Because pseudogout can closely resemble gout or septic arthritis, joint aspiration is often a very important part of the evaluation.
Sudden painful swollen joint
Large-joint involvement such as knee or wrist
Joint fluid showing CPP crystals
Imaging with chondrocalcinosis in the right setting
No evidence of septic arthritis on fluid testing and culture
Comorbidities & whole-body impact
CPPD can affect quality of life well beyond a single flare. Recurrent attacks can interrupt walking, sleep, work, exercise, and confidence with movement, and some patients also have coexisting osteoarthritis or chronic inflammatory symptoms between attacks. Clinicians may also look for associated metabolic conditions when CPPD occurs at a younger age or in unusual patterns.
- Recurrent flares causing loss of function
- Coexisting osteoarthritis or chronic joint damage
- Reduced walking or hand function depending on the joint involved
- Sleep disruption during severe attacks
- Need to evaluate metabolic contributors in selected patients
- Rare axial or atypical involvement in some forms of CPPD
Prognosis (what to expect long-term)
Pseudogout is often manageable, but the long-term course varies. Some patients have only occasional flares, while others have recurrent attacks or chronic inflammatory symptoms that resemble another type of arthritis. The goal is to treat acute flares quickly, reduce recurrence when possible, preserve joint function, and identify any contributing metabolic or structural factors.
Acute attacks can be very painful but are often treatable.
Some patients have long quiet periods between flares.
Others need longer-term planning because attacks return or chronic inflammation develops.
Understanding Pseudogout: Complete Disease Explanation
Pseudogout happens when calcium pyrophosphate crystals deposit in cartilage and other joint tissues, then trigger inflammation. Once the immune system reacts, the joint lining becomes inflamed and the attack can resemble gout or infection. CPPD is the broader disease category, while pseudogout refers specifically to the acute flare pattern that many patients experience.
What happens inside the joint?
In CPPD, crystals form and deposit inside the joint, often in cartilage. When those crystals shed or trigger immune activation, inflammatory cells enter the joint and create swelling, warmth, pain, and stiffness. This crystal-driven inflammation is why symptoms can come on suddenly even if the joint seemed stable beforehand.
Calcium pyrophosphate crystal deposition → immune activation in the joint → acute inflammation → hot swollen painful attack.
Pseudogout vs gout
Pseudogout and gout are both crystal arthritides, but they are caused by different crystals. Gout is caused by monosodium urate crystals related to uric acid, while pseudogout is caused by calcium pyrophosphate crystals. They can look very similar during an acute flare, which is why joint-fluid analysis is often the best way to tell them apart.
Gout and pseudogout are treated differently over the long term.
Uric-acid lowering therapy helps gout, but it does not treat CPPD crystals.
Correct diagnosis helps avoid unnecessary or ineffective long-term medication.
Diagnosis: exam, labs, imaging
Pseudogout is diagnosed using the overall clinical picture, joint aspiration, crystal analysis, and supportive imaging. Joint-fluid testing is especially important because it can identify calcium pyrophosphate crystals and help exclude infection. X-rays, ultrasound, or other imaging may show chondrocalcinosis or other changes consistent with CPPD, but imaging alone does not fully replace joint-fluid analysis during a concerning acute flare.
Tests often ordered during initial evaluation
Tests help confirm the diagnosis, exclude infection, and identify associated conditions.
- Joint aspiration to look for CPP crystals and send fluid for Gram stain and culture.
- X-rays or ultrasound to look for chondrocalcinosis and joint changes.
- Blood tests when clinicians need to evaluate inflammation, infection risk, or metabolic contributors.
- Selected laboratory screening for conditions such as hemochromatosis, magnesium abnormalities, calcium or parathyroid disorders in appropriate cases.
Treatment: flare control + long-term management
Effective pseudogout treatment has two main goals: control the acute flare quickly and reduce recurrence or chronic inflammation over time when needed. Common treatments for a flare include NSAIDs when safe, colchicine, corticosteroids, or joint aspiration and steroid injection depending on the clinical situation. Long-term management focuses on preventing repeat attacks in selected patients, managing any underlying metabolic contributors, and protecting the affected joint.
1) Flare control (short-term relief)
Acute pseudogout is usually treated with anti-inflammatory therapy. NSAIDs, colchicine, and corticosteroids are all commonly used, and some patients improve more quickly after aspiration of a tense swollen joint or an intra-articular steroid injection. The safest option depends on kidney function, bleeding risk, stomach history, infection concern, and the number of joints involved.
2) Long-term management (preventing recurrence)
Some patients with recurrent attacks benefit from low-dose colchicine or other preventive strategies. Long-term care may also include identifying and treating associated metabolic disorders, managing coexisting osteoarthritis, and adjusting activity during or after flares. Unlike gout, there is no uric-acid lowering treatment for CPPD because the underlying crystals are different.
3) Lifestyle strategies that support treatment
- Rest the affected joint during severe flares, then return to movement gradually as inflammation settles.
- Use ice or cold packs if recommended to reduce pain and swelling during acute attacks.
- Keep follow-up appointments if attacks are recurrent or if your clinician is evaluating metabolic contributors.
- Track which joints flare, how long attacks last, and whether there are triggers such as illness, surgery, or trauma.
- Address coexisting osteoarthritis or mobility limits to protect long-term joint function.
Treatment targets (pain, inflammation, recurrence)
In pseudogout, treatment targets focus on stopping the acute inflammatory attack, relieving joint pain, restoring movement, and reducing future flares when possible. Clinicians track the frequency of attacks, the joints involved, response to anti-inflammatory treatment, and whether chronic symptoms or structural joint disease are developing. Good control means shorter flares, safer movement, and fewer interruptions to daily life.
| Target area | What your clinician tracks | What “on target” can look like |
|---|---|---|
| Acute pain and swelling | Redness, warmth, tenderness, flare severity, ability to bear weight or use the joint | Rapid symptom relief and easier joint movement |
| Inflammation control | Joint response to treatment, recurrence pattern, fluid findings when needed | Shorter attacks and fewer severe episodes |
| Long-term joint health | Chronic symptoms, OA overlap, function, mobility, metabolic contributors | Better joint function and lower recurrence burden |
Case Study 1 (Example)
Patient developed sudden joint pain and swelling in the knee with warmth and limited movement. Evaluation suggested pseudogout rather than uric- acid gout or joint infection.
Pseudogout vs septic arthritis (quick table)
Pseudogout and septic arthritis can both cause a very hot swollen painful joint, which is why this distinction is so important. Septic arthritis is a joint infection and can destroy the joint quickly, while pseudogout is a crystal-triggered inflammatory flare. In real clinical practice, doctors often need joint aspiration and culture to separate the two safely.
| Feature | Pseudogout | Septic arthritis |
|---|---|---|
| Main cause | Calcium pyrophosphate crystals | Infection inside the joint |
| Presentation | Sudden hot swollen painful joint | Also sudden hot swollen painful joint |
| Joint fluid | CPP crystals may be present | Bacteria may be found on Gram stain or culture |
| Urgency | Urgent evaluation needed | Medical emergency |
| Treatment | Anti-inflammatory treatment | Urgent antibiotics and drainage |
When to seek urgent care
- Hot swollen joint with fever, severe illness, or inability to bear weight, because infection must be ruled out urgently.
- Sudden severe joint swelling that is rapidly worsening or very different from past flares.
- Major redness, chills, or symptoms suggesting septic arthritis rather than a routine crystal flare.
- Repeated attacks, new joint involvement, or symptoms that do not improve with usual treatment.
Call Now for Pseudogout Care
⭐ Google Rating: 4.7/5 (184 reviews) • Insurance accepted: Most major plans (verify with office).
Patient testimonial: “My knee became swollen and painful overnight. The team explained what pseudogout was, ruled out infection, and helped me get relief quickly.”
Call Now: (352) 717-0603 Request AppointmentClinic Address
Rheumatology Care Associates PLLC (RCA)
2611 S US Hwy 27, Clermont, FL 34711
Email: info@rheumatologycareassociates.com
Office hours: Mon 8:30AM–5:00PM; Tue 8:30AM–5:00PM; Wed 8:00AM–3:30PM; Thu 8:30AM–5:00PM; Fri 9:00AM–1:30PM.
FAQ
Conclusion
Pseudogout is a treatable crystal arthritis that can cause sudden severe joint inflammation and major short-term loss of function if not recognized promptly. If you develop a hot swollen painful joint, especially in the knee or wrist, a rheumatology or urgent medical evaluation can help confirm the diagnosis, rule out infection, and start the right treatment.
Disclaimer: This article is for educational purposes and does not replace professional medical advice. Always seek urgent care for a hot swollen joint, especially with fever or severe illness.
© 2026 Rheumatology Care Associates. All rights reserved.