Medically reviewed by Dr. Priya Prakash (Rheumatologist, board certified) | Last updated: March 20, 2026
What Is Eosinophilic Granulomatosis with Polyangiitis (EGPA)? Symptoms, Causes, Diagnosis & Treatment
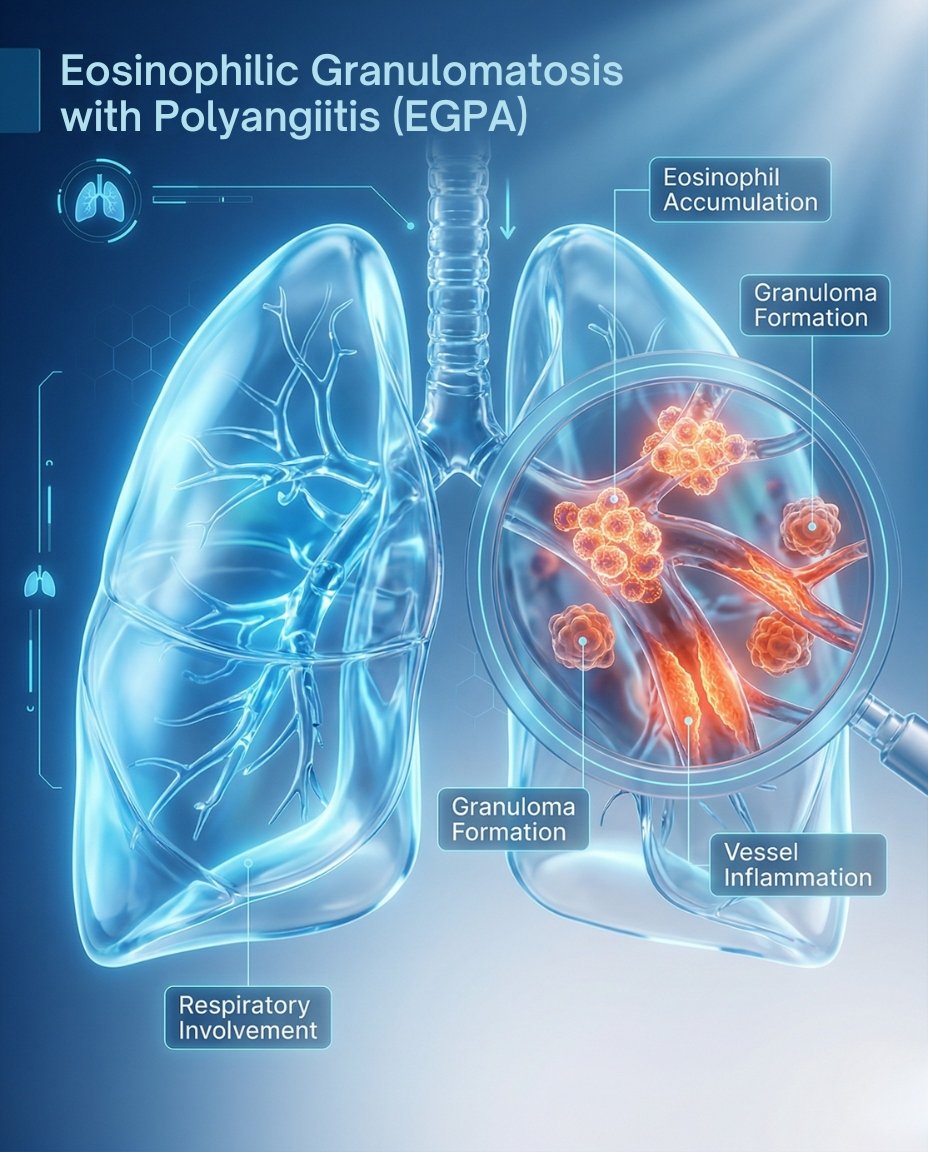
Eosinophilic granulomatosis with polyangiitis (EGPA) is a rare autoimmune vasculitis that causes inflammation of small blood vessels. It is strongly associated with asthma, eosinophilia, sinus disease, and inflammatory damage that can involve the lungs, nerves, skin, heart, digestive tract, kidneys, and other organs. Early diagnosis and treatment are important because some forms of EGPA can become organ-threatening or life-threatening without prompt care.
If you’re searching what is EGPA, the simplest answer is that it is a rare form of vasculitis in which inflammation and high eosinophil activity damage blood vessels and tissues throughout the body. Many patients have a background of asthma, allergies, nasal polyps, or sinus problems before the vasculitis becomes obvious. A rheumatologist can help confirm the diagnosis and create an individualized EGPA treatment plan based on organ involvement, eosinophil burden, vasculitic features, and whether the disease is mild, relapsing, or severe.
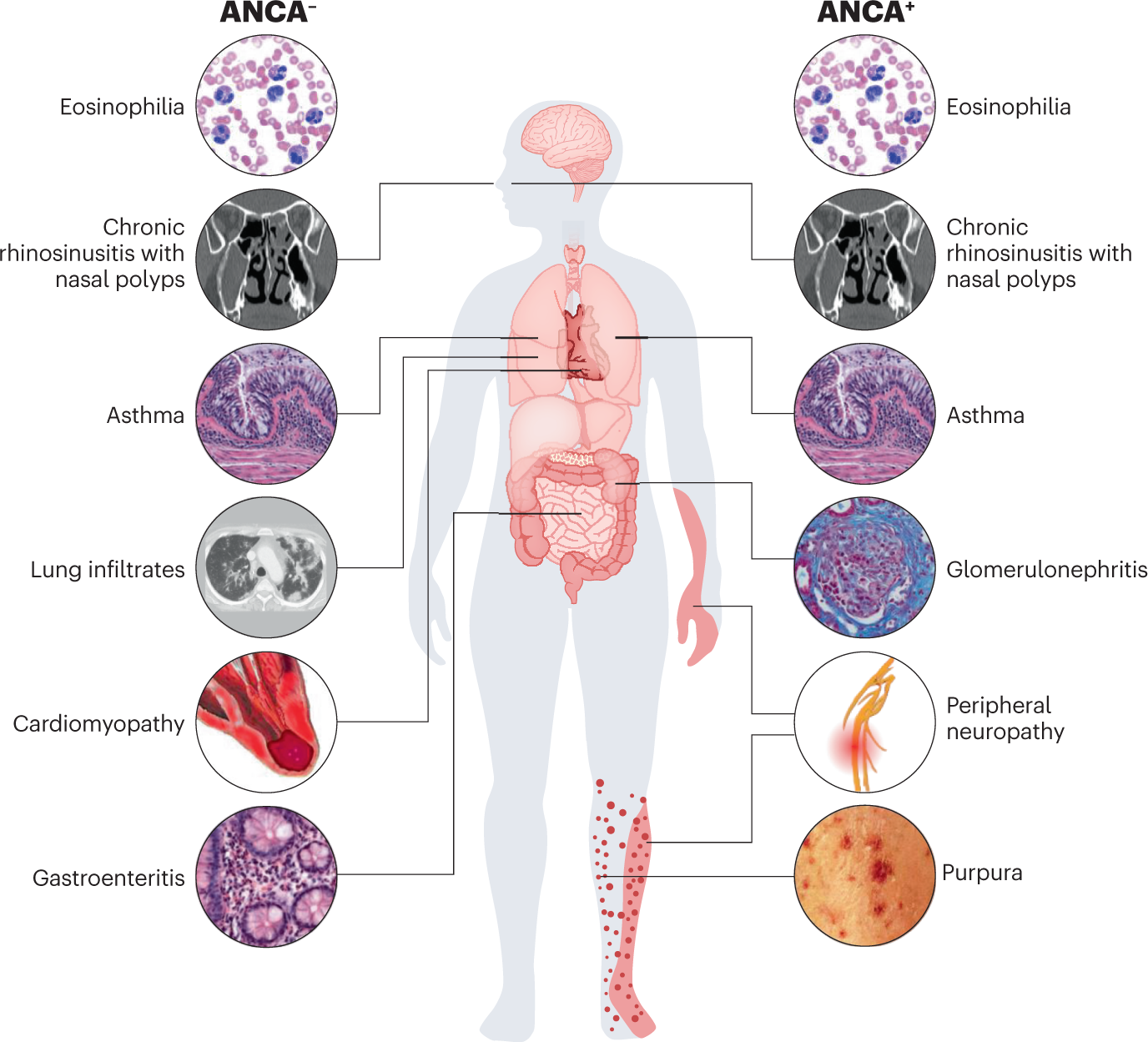
EGPA was formerly called Churg-Strauss syndrome and is one of the ANCA-associated vasculitides, although ANCA is not present in every patient. Some patients have more vasculitic features such as neuropathy, purpura, or kidney involvement, while others have more eosinophilic features such as lung, heart, or gastrointestinal disease. Because EGPA can mimic asthma complications, eosinophilic lung disease, infection, drug reactions, or other vasculitides, getting the diagnosis right matters.
Table of Contents
- What Is EGPA? Simple medical definition
- EGPA at a glance
- Common EGPA patterns
- EGPA symptoms (what it feels like)
- Causes & risk factors
- How EGPA is recognized
- Comorbidities & whole-body impact
- Prognosis (what to expect long-term)
- Understanding EGPA: complete disease explanation
- EGPA vs granulomatosis with polyangiitis
- Diagnosis: exam, labs, testing
- Treatment: symptom relief + long-term disease control
- Treatment targets (eosinophils, vasculitis, organ protection)
- EGPA vs severe eosinophilic asthma (quick table)
- When to seek urgent care
- Downloadable EGPA symptom checklist
- Related conditions (internal links)
- FAQs
- Conclusion + next steps
What Is EGPA? Simple Medical Definition
Eosinophilic granulomatosis with polyangiitis (EGPA) is a rare systemic necrotizing small-vessel vasculitis associated with asthma, eosinophilia, and eosinophil-rich inflammation. In short, clinically, what is EGPA? It is a multisystem autoimmune vasculitis in which eosinophilic tissue injury and blood-vessel inflammation can damage the lungs, nerves, skin, heart, gastrointestinal tract, kidneys, and other organs.
EGPA at a Glance
Asthma history common Many patients already have asthma or chronic sinus disease
High eosinophils Blood eosinophilia is a major clue
Small-vessel vasculitis Blood-vessel inflammation can damage multiple organs
Nerve problems possible Numbness, weakness, or foot drop may occur
Heart involvement matters Cardiac disease can be serious and sometimes life-threatening
EGPA is more than asthma with high eosinophils. It is a systemic vasculitis that can become organ-threatening if not recognized early.
Common EGPA Patterns
EGPA can present with more eosinophilic disease, more vasculitic disease, or a mixed pattern. Some patients mainly have asthma, sinus disease, lung infiltrates, and eosinophilic inflammation, while others show stronger vasculitic features such as neuropathy, purpura, or kidney involvement. Clinicians also consider whether a patient is ANCA-positive or ANCA-negative because that can correlate with different complication patterns.
Airway-dominant EGPA Asthma, nasal polyps, sinus disease, and eosinophilic lung features dominate
Vasculitic EGPA Neuropathy, purpura, kidney disease, and systemic vasculitis are more prominent
Cardiac or GI EGPA Heart or digestive tract involvement becomes a major concern
ANCA-positive EGPA Vasculitic manifestations may be more common
ANCA-negative EGPA Eosinophilic tissue involvement such as heart or GI disease may be more common
EGPA symptoms (what it feels like)
Typical EGPA symptoms include asthma worsening, sinus disease, nasal polyps, fatigue, fever, weight loss, numbness, weakness, and lung symptoms. Many patients also develop skin rash, purpura, shortness of breath, cough, chest symptoms, abdominal pain, diarrhea, muscle pain, or tingling in the hands and feet. Some people notice foot drop, hand weakness, or severe burning nerve pain when peripheral nerves are involved.
Lungs • Sinuses • Nose • Nerves • Skin • Heart • Digestive tract • Kidneys • Blood vessels
Asthma, allergies
Sinus disease
Inflammation
Tissue injury
Organ damage
Neuropathy, rash
Confirm EGPA
Protect organs
Wheel shows a simplified pathway: asthma and eosinophilic inflammation → blood-vessel injury → multisystem EGPA symptoms and organ-focused management.
Images for patient education
Asthma and sinus disease
Nerve and skin involvement
Heart and lung risk
Causes & risk factors
The exact cause of EGPA is not fully understood, but it involves abnormal immune activation, eosinophilic inflammation, and small-vessel vasculitis. Most patients have a history of asthma, allergic rhinitis, chronic sinusitis, or nasal polyps before systemic disease develops. ANCA is present in only a subset of patients, and the disease seems to reflect a mix of eosinophilic immune injury and vasculitic autoimmune damage rather than one single mechanism alone.
- Asthma or airway allergy history
- Chronic sinusitis or nasal polyps
- Marked eosinophilia on blood testing
- Small-vessel inflammation affecting multiple organs
- ANCA positivity in only some patients
- Risk of cardiac, nerve, lung, skin, or GI involvement
Evidence-based references (guidelines + high-quality sources)
General patient education: RheumInfo. Clinical overview: Vasculitis Foundation. Professional review: NIH/NCBI StatPearls.
How EGPA Is Recognized
EGPA is recognized through the combination of asthma or sinus disease, eosinophilia, systemic symptoms, and evidence of vasculitis or eosinophilic organ damage. Specialists often suspect EGPA when a patient with asthma develops neuropathy, rash, lung infiltrates, heart involvement, eosinophilia, or unexplained systemic illness. Diagnosis may require looking at the whole pattern over time because the disease can evolve in stages rather than showing all features at once.
Asthma and chronic sinus disease
Elevated eosinophils in blood or tissue
Lung infiltrates or eosinophilic respiratory disease
Neuropathy, especially mononeuritis multiplex or foot drop
Purpura or other vasculitic skin lesions
Cardiac, GI, renal, or other organ involvement in the right pattern
Comorbidities & whole-body impact
EGPA can affect quality of life through both chronic airway disease and systemic vasculitic injury. Patients may face severe asthma burden, chronic sinus symptoms, neuropathic pain, weakness, reduced mobility, cardiac complications, GI symptoms, and steroid-related treatment burden. Some of the most serious long-term issues involve the heart, peripheral nerves, lungs, and relapse risk.
- Severe asthma and chronic sinus disease
- Peripheral neuropathy with weakness, numbness, or foot drop
- Cardiac inflammation or cardiac damage risk
- Skin vasculitis or purpura
- Gastrointestinal pain or eosinophilic GI involvement
- Relapse risk and medication side-effect burden
Prognosis (what to expect long-term)
The long-term outlook in EGPA depends on which organs are involved and how quickly treatment begins. Many patients improve significantly with treatment, but relapses are common, and some forms of organ involvement, especially cardiac disease, can be serious. The central goals are to control eosinophilic inflammation, suppress vasculitis, prevent organ damage, and taper corticosteroids safely when possible.
Many patients respond well to treatment, but relapse monitoring remains important.
Heart, nerve, lung, and GI involvement strongly influence severity.
Long-term care often focuses on both disease control and reducing steroid burden.
Understanding EGPA: Complete Disease Explanation
EGPA combines two important processes: eosinophilic inflammation and vasculitis. Eosinophils can directly damage tissues such as the lungs, heart, and gastrointestinal tract, while vasculitis inflames blood vessels and disrupts blood flow to nerves, skin, kidneys, and other organs. This dual process explains why EGPA can look partly like severe eosinophilic asthma and partly like a multisystem vasculitis.
What happens in the body?
Many patients pass through overlapping phases that include airway allergy or asthma, eosinophilic inflammation, and then more obvious vasculitic disease. However, these phases do not always occur in a neat order, and some patients present with mixed features from the beginning. The final disease pattern depends on where eosinophils accumulate and which blood vessels become inflamed.
Asthma and eosinophilic immune activation → eosinophil-rich tissue injury → small-vessel vasculitis → nerve, lung, heart, skin, GI, or kidney involvement.
EGPA vs granulomatosis with polyangiitis
EGPA and granulomatosis with polyangiitis are both ANCA-associated vasculitides, but they are not the same disease. EGPA is much more strongly linked to asthma, eosinophilia, nasal polyps, and eosinophilic tissue injury, while granulomatosis with polyangiitis more classically affects the upper airway, lungs, and kidneys with granulomatous inflammation and often without the same eosinophilic pattern. This distinction matters because the symptom profile, lab clues, and treatment decisions can differ.
EGPA often begins with asthma and eosinophilia.
GPA more commonly presents with destructive ENT disease and kidney involvement without the same asthma-eosinophil pattern.
Correct diagnosis helps guide testing, biopsy decisions, and long-term treatment planning.
Diagnosis: exam, labs, testing
EGPA is diagnosed using the overall clinical pattern, blood eosinophil levels, ANCA testing, imaging, organ evaluation, and sometimes biopsy. Doctors may order CBC with differential, inflammatory markers, ANCA testing, IgE in some cases, chest imaging, pulmonary assessment, cardiac testing, nerve studies, urinalysis, and tissue biopsy when feasible. Biopsy can support the diagnosis, but it is not always required if the overall pattern strongly fits EGPA and other causes are excluded.
Tests often ordered during initial evaluation
Tests help confirm the diagnosis, rule out mimics, and define organ involvement.
- Blood tests including CBC with eosinophil count, inflammatory markers, ANCA, and selected immune markers.
- Chest imaging and pulmonary evaluation for lung infiltrates or airway disease.
- Cardiac evaluation when there is chest pain, shortness of breath, abnormal troponin, or suspected heart involvement.
- Nerve studies when weakness, numbness, or mononeuritis multiplex is suspected.
- Urinalysis and kidney-function testing to screen for renal involvement.
- Biopsy of skin, nerve, lung, or other tissue when feasible and clinically useful.
Treatment: symptom relief + long-term disease control
Effective EGPA treatment has two main goals: control active eosinophilic and vasculitic inflammation, and prevent permanent organ damage. Corticosteroids are commonly used early, and patients with more severe disease may also need immunosuppressive or biologic therapy depending on organ involvement and relapse risk. The treatment plan differs depending on whether the disease is mainly eosinophilic, mainly vasculitic, or clearly organ-threatening.
1) Symptom control (short-term relief)
Systemic corticosteroids are often the first treatment used to reduce active inflammation quickly. Asthma control, sinus care, and supportive symptom treatment remain important because airway disease is a major part of EGPA in many patients. In severe disease, rapid treatment is especially important when the heart, nerves, lungs, kidneys, or gastrointestinal tract are affected.
2) Long-term management (preventing relapse and organ damage)
Longer-term treatment may include immunosuppressive therapy or biologic treatment in selected patients, especially when disease is relapsing, severe, or steroid-dependent. Organ-threatening disease may require more aggressive induction therapy, while non-severe relapsing eosinophilic disease may be approached differently. Long-term follow-up usually includes monitoring eosinophils, asthma control, nerve recovery, cardiac safety, relapse pattern, and steroid side effects.
3) Lifestyle strategies that support treatment
- Report new numbness, weakness, foot drop, chest symptoms, or severe abdominal pain urgently.
- Keep asthma and sinus treatment optimized because airway disease often remains part of the illness even when vasculitis is controlled.
- Track flares carefully, including steroid needs, eosinophil trends, and organ-specific symptoms.
- Attend regular follow-up for heart, nerve, lung, and medication-safety monitoring.
- Protect bone and infection risk when long steroid courses are required.
Treatment targets (eosinophils, vasculitis, organ protection)
In EGPA, treatment targets focus on reducing eosinophilic inflammation, suppressing vasculitis, controlling asthma and sinus disease, and protecting organs. Clinicians track symptoms, eosinophil counts, ANCA context, asthma burden, nerve function, cardiac status, lung findings, and relapse frequency. Good control means not only fewer flares, but also lower steroid burden and better long-term organ safety.
| Target area | What your clinician tracks | What “on target” can look like |
|---|---|---|
| Eosinophilic activity | Eosinophil counts, asthma control, sinus symptoms, lung infiltrates | Lower eosinophilic burden and better airway control |
| Vasculitis control | Skin lesions, neuropathy, inflammatory markers, relapse pattern | Less active vasculitic damage and fewer relapses |
| Organ protection | Heart, nerves, kidneys, lungs, GI symptoms, treatment safety | Stable organ function and safer long-term management |
Case Study 1 (Example)
Patient with long-standing asthma developed sinus problems, fatigue, and numbness in the limbs. Evaluation suggested EGPA rather than chronic- allergy or uncontrolled asthma alone.
EGPA vs severe eosinophilic asthma (quick comparison)
EGPA can resemble severe eosinophilic asthma, especially early on, but the two are not the same. Severe eosinophilic asthma mainly affects the airways, while EGPA adds systemic vasculitis or eosinophilic organ injury involving nerves, skin, heart, GI tract, kidneys, or other tissues. Distinguishing between them matters because EGPA needs broader organ evaluation and often more systemic treatment planning.
| Feature | EGPA | Severe eosinophilic asthma |
|---|---|---|
| Asthma | Usually present | Present |
| Eosinophilia | Common and often marked | Can also occur |
| Vasculitis | Yes | No systemic vasculitis |
| Neuropathy, purpura, cardiac or GI disease | May occur | Not typical as part of asthma alone |
| Workup | Needs multisystem vasculitis evaluation | Mainly airway-focused evaluation |
When to seek urgent care
- Chest pain, fainting, severe shortness of breath, or other signs of possible cardiac involvement.
- New weakness, foot drop, severe numbness, or rapidly progressive neuropathy.
- Severe abdominal pain, GI bleeding symptoms, or signs of intestinal involvement.
- Rapid overall worsening, skin necrosis, kidney symptoms, or severe systemic illness.
Call Now for EGPA Care
⭐ Google Rating: 4.7/5 (184 reviews) • Insurance accepted: Most major plans (verify with office).
Patient testimonial: “I thought it was only asthma and sinus trouble until the numbness and abnormal blood counts started. The team recognized the larger EGPA picture and helped me get the right evaluation.”
Call Now: (352) 717-0603 Request AppointmentClinic Address
Rheumatology Care Associates PLLC (RCA)
2611 S US Hwy 27, Clermont, FL 34711
Email: info@rheumatologycareassociates.com
Office hours: Mon 8:30AM–5:00PM; Tue 8:30AM–5:00PM; Wed 8:00AM–3:30PM; Thu 8:30AM–5:00PM; Fri 9:00AM–1:30PM.
Related conditions (internal links)
FAQ
Conclusion
EGPA is a rare but treatable vasculitis that combines eosinophilic inflammation with blood-vessel injury and can affect many organs. If you have asthma together with high eosinophils, sinus disease, rash, numbness, weakness, chest symptoms, or unexplained systemic illness, a rheumatology evaluation can help confirm the diagnosis and start the right organ-protective treatment plan.
Disclaimer: This article is for educational purposes and does not replace professional medical advice. Always seek prompt care for chest pain, neuropathy, severe abdominal pain, or signs of organ-threatening disease.
© 2026 Rheumatology Care Associates. All rights reserved.