What Is Ankylosing Spondylitis (AS)? Symptoms, Causes, Diagnosis & Treatment
Ankylosing spondylitis (AS) is a chronic inflammatory arthritis that mainly affects the spine and sacroiliac (SI) joints. It often causes inflammatory back pain, morning stiffness, and reduced mobility, and may also affect the hips, shoulders, chest wall, and eyes. Early diagnosis and treatment can reduce pain, preserve mobility, and lower the risk of long-term stiffness.
If you’re searching what is ankylosing spondylitis, the simplest answer is that AS is a long-term inflammatory arthritis that usually starts in the lower back or buttock area. Symptoms often feel worse after rest and better with movement, which is a key inflammatory pattern. A rheumatologist can confirm AS and create an individualized ankylosing spondylitis treatment plan based on symptoms, exam, labs, and imaging.
Spondylitis
Many people notice persistent low back pain, morning stiffness, buttock pain, or reduced flexibility. AS can also cause fatigue, hip pain, chest wall tightness, or eye inflammation called uveitis. Because it can resemble mechanical back pain or other conditions, getting the diagnosis right matters.
Table of Contents
- What Is Ankylosing Spondylitis? Simple medical definition
- AS at a glance
- Axial spondyloarthritis patterns
- Ankylosing spondylitis symptoms (what it feels like)
- Causes & risk factors
- How AS is recognized
- Comorbidities & whole-body risk
- Prognosis (what to expect long-term)
- Understanding AS: complete disease explanation
- AS vs psoriatic arthritis
- Diagnosis: exam, labs, imaging
- Treatment: symptom relief + disease control
- Treatment targets (maintaining mobility)
- Ankylosing spondylitis vs rheumatoid arthritis (quick table)
- When to seek urgent care
- Downloadable AS symptom checklist
- Related conditions (internal links)
- FAQs
- Conclusion + next steps
What Is Ankylosing Spondylitis? Simple Medical Definition
Ankylosing spondylitis (AS) is a chronic inflammatory arthritis that mainly affects the spine and sacroiliac joints. In short, clinically, what is AS? It’s an immune-driven inflammatory disease that can cause back pain, stiffness, fatigue, and reduced spinal mobility, and over time may lead to structural changes if inflammation is not controlled.
AS at a Glance
Inflammatory back pain Often worse with rest, better with movement
Morning stiffness Common in lower back and hips
SI joint pain Buttock or deep low back discomfort
Reduced flexibility Trouble bending, twisting, or standing upright
Uveitis Red painful eye in some patients
Symptoms may flare and settle, but ongoing inflammation can still affect posture and mobility.
Axial Spondyloarthritis Patterns
AS is part of the axial spondyloarthritis family, which mainly affects the spine and sacroiliac joints. Clinicians often describe the pattern based on whether disease is mostly spinal, whether hips or shoulders are involved, and whether eye or bowel inflammation is present.
Predominantly axial disease Spine and SI joints are the main areas
Peripheral joint involvement Hips, shoulders, or knees may also be affected
Enthesitis pattern Pain where tendons attach to bone
Extra-articular disease Eyes or bowel inflammation may occur
Progressive stiffness Long-term disease can reduce flexibility
Ankylosing spondylitis symptoms (what it feels like)
Typical ankylosing spondylitis symptoms include chronic low back pain, morning stiffness, buttock pain, and symptoms that improve with movement. Many people also have fatigue, reduced flexibility, and pain in the hips, shoulders, or chest wall. Some patients develop uveitis, which causes a red painful eye, light sensitivity, or blurry vision.
Low back/SI joints • Buttocks • Hips • Chest wall • Shoulders • Heel/Achilles • Eyes
Genetics
Family history
SI joints
Spine
Pain, stiffness
Less mobility
Confirm diagnosis
Treatment plan
Wheel shows a simplified pathway: risk factors → spine inflammation → symptoms → evaluation and long-term control.
Images for patient education
AS back pain

AS inflammation
AS symptom areas
Causes & risk factors
AS is driven by immune-system inflammation for reasons that are not fully understood. It often begins around the joints between the spine and pelvis, and risk is influenced by genetics and family history. It is not simply wear-and-tear back pain.
- Chronic inflammatory low back pain
- Morning stiffness that improves with movement
- Family history of AS or spondyloarthritis
- Buttock or sacroiliac joint pain
- Uveitis or enthesitis history
Evidence-based references (guidelines + high-quality sources)
General patient education: NIH/NIAMS. Patient overview and disease explanation: RheumInfo. Diagnosis and treatment overview: NIAMS diagnosis & treatment.
How AS Is Recognized
Ankylosing spondylitis is recognized as part of axial spondyloarthritis, a group of inflammatory conditions centered on the spine and sacroiliac joints. Specialists look for inflammatory back pain, reduced spinal mobility, imaging changes, and related inflammatory features rather than relying on one lab result alone.
Chronic inflammatory low back pain
Morning stiffness that improves with activity
Sacroiliac inflammation on imaging
Reduced spinal mobility or posture change
Uveitis, enthesitis, or family history
Comorbidities & whole-body risk
Ankylosing spondylitis is not only a spine disease. Some patients also have eye inflammation, bowel inflammation, hip involvement, or major stiffness that affects posture and daily function. Good AS care looks beyond pain alone and considers the broader effects of chronic inflammation.
- Uveitis (urgent red painful eye, light sensitivity, blurry vision)
- Reduced spinal flexibility and posture changes
- Hip or shoulder involvement affecting mobility
- Fatigue and sleep disruption
- Inflammatory bowel disease overlap in some patients
- Functional limitation if disease stays active
Prognosis (what to expect long-term)
AS is usually a long-term inflammatory condition, but severity varies from person to person. Some people remain fairly stable, while others develop progressive stiffness over time. The goal is to control inflammation early so the spine stays as flexible and functional as possible.
Early treatment can improve pain and mobility.
Without good control, AS can reduce spinal flexibility over time.
Many patients do better with medication, exercise, posture work, and regular follow-up.
Understanding AS: Complete disease explanation
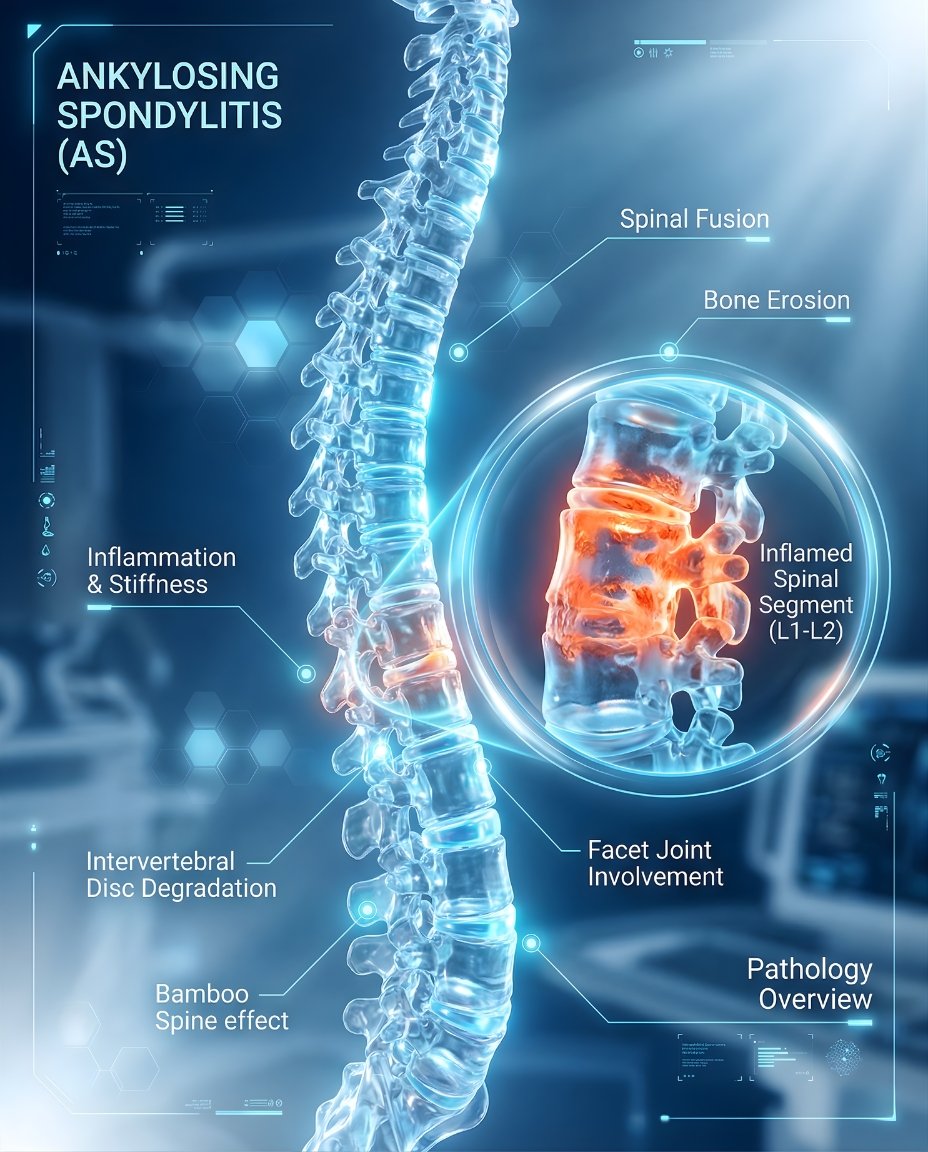
AS happens when inflammatory activity targets the sacroiliac joints, spine, and sometimes other joints or tendon attachment sites. Over time, uncontrolled inflammation can contribute to chronic pain, stiffness, fatigue, reduced motion, and structural spinal change. A complete evaluation often looks for features beyond the back alone.
What happens at the tissue level?
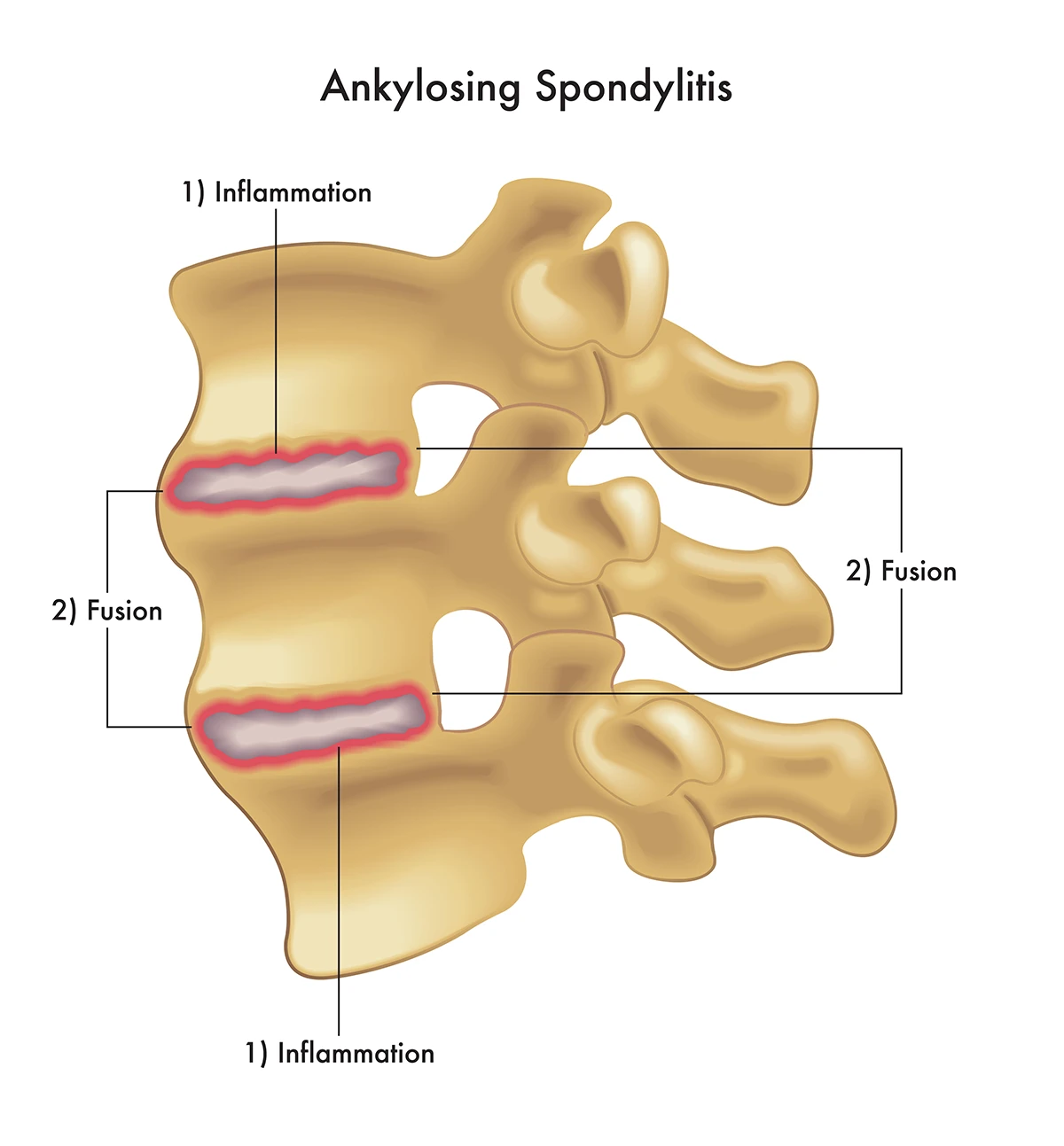
In AS, inflammation often starts around the sacroiliac joints and spinal structures, and may also involve entheses where tendons and ligaments attach to bone. This helps explain why symptoms include inflammatory back pain, stiffness after rest, and gradual loss of flexibility.
Genetic tendency + immune inflammation → SI joint/spine inflammation → pain and stiffness → possible structural change without control.
AS vs psoriatic arthritis
Both ankylosing spondylitis and psoriatic arthritis are part of the spondyloarthritis spectrum and can cause inflammatory back pain. AS more classically centers on the spine and sacroiliac joints, while psoriatic arthritis is more often linked with psoriasis, nail disease, dactylitis, and peripheral joint patterns.
Treatment choices may differ depending on whether spine symptoms, peripheral joints, psoriasis, eye disease, or bowel disease are dominant.
A correct diagnosis helps match therapy to the main disease pattern.
Diagnosis: exam, labs, imaging
AS is diagnosed using the overall pattern: symptoms, physical exam, inflammatory features, and imaging findings. There is no single definitive blood test for AS, so clinicians combine the history of inflammatory back pain with exam findings and imaging of the SI joints and spine.
Tests often ordered during initial evaluation
Tests help support the diagnosis, assess inflammation, and guide treatment planning.
- Inflammation markers (ESR/CRP) to look for inflammatory activity.
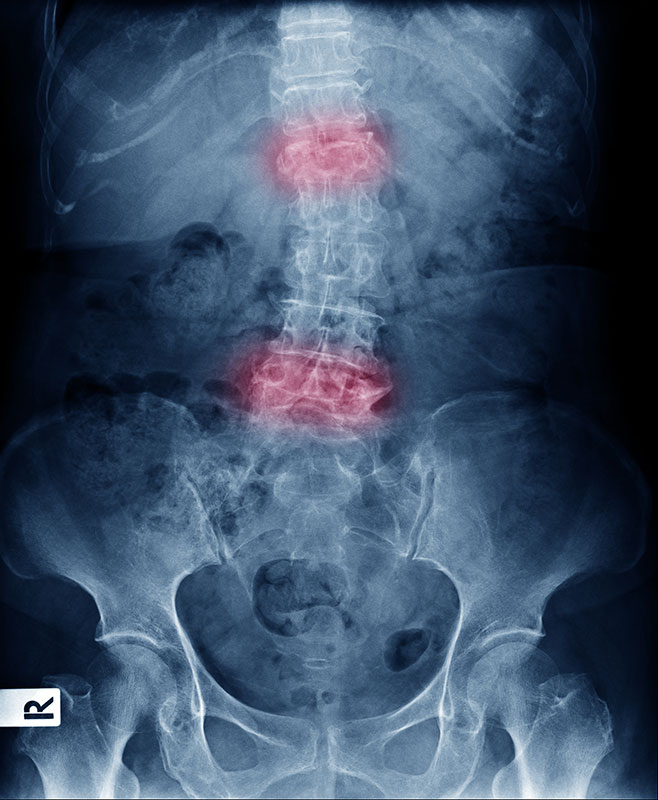
- Imaging of the sacroiliac joints and spine, often with X-rays and sometimes MRI.
- Baseline blood counts and liver/kidney tests before certain medications.
- Additional evaluation when symptoms suggest uveitis, bowel inflammation, or overlap disease.
Treatment: symptom relief + disease control
Effective ankylosing spondylitis treatment has two main goals: reduce pain and stiffness now, and preserve flexibility and function over time. Standard care often combines medication with physical therapy and regular exercise, because movement is central to maintaining mobility.
1) Symptom control (short-term relief)
Short-term relief may include anti-inflammatory medication to reduce pain and stiffness. The safest option depends on the patient’s stomach, kidney, blood pressure, and other health factors.
2) Disease control (preventing progression)
If AS remains active or function-limiting, long-term therapy may include biologic or other targeted treatment. Treatment decisions depend on disease severity, mobility limits, imaging findings, and whether uveitis or other inflammatory features are present.
3) Lifestyle strategies that support treatment
- Use regular exercise and stretching to preserve mobility and reduce stiffness.
- Work on posture and spinal extension habits as advised by your clinician or therapist.
- Stay active, because rest alone usually worsens inflammatory stiffness.
- Prioritize sleep and symptom management to reduce fatigue and improve daily function.
Treatment targets (maintaining mobility)
In AS, treatment targets focus on lowering inflammation, improving pain and stiffness, and preserving movement, posture, and daily function. This means clinicians track symptoms and mobility over time, not pain alone.
| Target area | What your clinician tracks | What “on target” can look like |
|---|---|---|
| Back pain and stiffness | Morning stiffness, night pain, daily function | Less stiffness, better movement, better sleep |
| Spinal mobility | Flexibility, posture, range of motion | Maintained mobility and less decline |
| Whole-body inflammation | Flares, fatigue, eye/bowel symptoms | Fewer flares and better control |
Case Study 1 (Example)
Patient had progressive morning stiffness, inflammatory anti-low back pain, and buttock pain that improved with movement. Evaluation suggested inflammatory axial arthritis consistent with ankylosing spondylitis…
Ankylosing spondylitis vs rheumatoid arthritis (quick comparison)
AS and rheumatoid arthritis can both cause inflammatory pain and stiffness, but AS more classically centers on the spine and sacroiliac joints. Rheumatoid arthritis more often affects small peripheral joints, while AS is more associated with inflammatory back pain and reduced spinal mobility.
| Feature | Ankylosing spondylitis (AS) | Rheumatoid arthritis (RA) |
|---|---|---|
| Main location | Spine and sacroiliac joints | Small peripheral joints more typical |
| Pain pattern | Often worse after rest, better with movement | Inflammatory stiffness but less classically axial |
| Mobility effect | Reduced spinal flexibility may occur | Hand and foot function more often affected |
| Imaging focus | SI joints and spine | Peripheral erosive joint disease |
When to seek urgent care
- Red, painful eye with light sensitivity or blurry vision (possible uveitis).
- New neurologic symptoms such as weakness, numbness, or bowel/bladder changes.
- Severe chest pain or shortness of breath that is new or unexplained.
- Rapid decline in mobility or severe unexplained worsening.
Call Now for Ankylosing Spondylitis Care
⭐ Google Rating: 4.7/5 (184 reviews) • Insurance accepted: Most major plans (verify with office).
Patient testimonial: “My back stiffness kept getting worse. The team explained what AS is, reviewed my options, and helped me move more comfortably.”
Call Now: (352) 717-0603 Request AppointmentClinic Address
Rheumatology Care Associates PLLC (RCA)
2611 S US Hwy 27, Clermont, FL 34711
Email: info@rheumatologycareassociates.com
Office hours: Mon 8:30AM–5:00PM; Tue 8:30AM–5:00PM; Wed 8:00AM–3:30PM; Thu 8:30AM–5:00PM; Fri 9:00AM–1:30PM.
Related conditions (internal links)
FAQ
Conclusion
Ankylosing spondylitis is a treatable inflammatory arthritis that mainly affects the spine and sacroiliac joints, and it is often easier to manage when recognized early. If you have persistent morning stiffness, inflammatory back pain, buttock pain, reduced flexibility, or episodes of a red painful eye, a rheumatology evaluation can help clarify the diagnosis and next steps.
Disclaimer: This article is for educational purposes and does not replace professional medical advice. Always consult with your existing healthcare provider before starting new treatments. Dr. Priya Prakash and Rheumatology Care Associates are committed to evidence-based, personalized care.
© 2026 Rheumatology Care Associates. All rights reserved.